Mostly cholesterol stones (80%), pigment stones or mixed stones.
Whether cholesterol remains as solution within bile depends on it's concentration, and the levels of phospholipids and bile acids within.
If the bile is supersaturated by cholesterol, and/or levels of phospholipids and bile acids is low, this promotes formation of cholesterol crystals.
These cholesterol crystals are toxic towards the gall bladder musculature, and hence damages it.
This results in gall bladder hypomotility, and enhances the nucleation of theses gall bladder crystals.
Eventually, gall stones are formed.
As for pigment stones, there are 2 types, namely black and brown stones.
Black stones are sterile stones, usually caused by extensive hemolysis leading to unconjugated hyperbilirubinemia. Eg, seen in Hereditary Spherocytosis, Sickle-cell disease.
Whilst brown stones are non-sterile stones, mainly caused by infection.
Eg, certain bacteria (E.coli) produces B-glucoronidase, which converts conjugated bilirubin back to unconjugated bilirubin.
Also associated with parasitic worm infestation, eg : Ascariasis, Clonorchis sinensis
Complications
1) Gall bladder
Biliary colic
Acute cholecystitis
Chronic cholecystitis
Empyema
Mucocele
Perforation
2) Biliary tract
Biliary tract obstruction
Acute pancreatitis
Ascending cholangitis
3) Intestine
Gall stone ileus
Acute cholecystitis
Usually caused by obstruction of cystic duct by gall stones, leading to gall bladder distension, chemical inflammation, and eventual bacterial infection.
History
Age : Typically 30-60 years old. Presentation in younger patients, may be due to Congenital hemolytic anemia
Gender : Females are more commonly affected
Symptoms :
Fever
Sudden onset of severe, continuous RHC pain
Radiates to the back (close to the inferior angle of right scapula)
Associated with nausea and vomiting
Duration of pain usually exceeds 3-6 hours
Pain aggravated by movements and breathing
May have previous h/o of flatulent dyspepsia or biliary colic
On general examination :
Patient appears ill
Lying still on bed, breathing shallowly
Tachycardia +ve, Pyrexia +ve
During initial stages of inflammation - RHC fullness (known as Zackary-cope's sign)
RHC tenderness, guarding/rigidity, +ve Murphy's sign
Before the onset of guarding, during the early stages the gall bladder may be palpable
If the inflammation persisted for a few days, with subsequent subside of symptoms, an inflammatory mass may be palpable (empyema)
Boas Sign +ve
Biliary colic
Before proceeding to investigations of Acute cholecystitis, briefly about biliary colic.
It's actually a misnomer, caused by spasm of gall bladder musculature, trying to force the stone down the cystic duct.
Since it's a visceral pain, pain is usually felt over the epigastrium (foregut)
The pain is typically aggravated by intake of oily food.
Since after ingesting oily food, as it passes through the 2nd part of duodenum, it stimulates the production of cholecystikinin from the duodenal mucosa.
It causes contraction of the gall bladder musculature over the stones, hence causing pain.
Duration of pain typically lasted < 3 hours.
However, in practice, patient usually localizes their pain poorly (c/c usually diffuse upper abdominal pain)
It's a pseudocolic, since there's no complete relief of pain in between periods of excruciating exacerbations.
There might be nausea and vomiting.
On examination, there may be tachycardia, but fever is absent.
On abdominal examination, other than tenderness, guarding, usually there's no other signs.
Hence, there's a frequent overlap in between the clinical features of biliary colic and acute cholecystitis.
Here the table showing their difference :

Full blood count - reveals leucocytosis
Abdominal X ray - not useful, only 10-15% of the calculus is visible through plain abdominal X ray
USG abdomen - visualisation of gall bladder wall, contents, biliary tree
Management
As for asymptommatic gall stones, which is usually detected incidentally, the best option is to observe (no further intervention)
However, prophylactic cholecystectomy will be indicated in :
a) Non-functioning gall bladder
b) Gall bladder with calcified/thickened wall
c) Diabetic patients (prevent Emphysematous Cholecystitis)
d) Multiple small stones (risk of stones rolling into CBD)
e) Congenital hemolytic anemia
During acute presentation, > 90% of the cases, symptoms subsides with conservative management :
1) Nil by mouth
2) Administration of analgesics
3) Administration of antibiotics (Unasyn + Flagyl)
4) Gain IV access, give IV fluids
5) Monitoring of vital signs
6) If symptoms subsided, initially oral fluid intake is allowed, then followed by fat-free diet, and lastly regular diet
7) USG - to evaluate whether there's any local complications
8) Plan for cholecystectomy
Pre-operative investigations
1) Informed consent
2) Full blood count
3) BUSE/Creatinine
4) Liver function test
5) ECG, Chest X ray (if medically indicated)
6) Antibiotic prophylaxis
7) DVT prophylaxis
Cholecystectomy can be done via laproscopic approach or laparotomy.
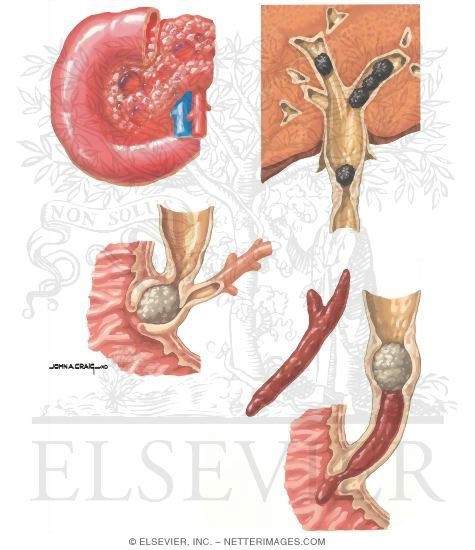
Gall stone ileus
Small bowel obstruction caused by gall stone impaction at the distal ileum
Usually seen in females, age > 60 years old, with h/o of recurrent cholecystitis
Erosion of the stones through the duodenum, eventually forming a fistula with the distal ileum
Presentation is similar to any other small bowel obstruction
Plain abdominal X ray reveals multiple air-fluid levels, and there might be aerobilia (gas within biliary tree)

Hard stones requires enterotomy
Mirizzi's syndrome

Gall stone impaction occurs at cystic duct.
There's impingement of the gall stone over the common hepatic duct, which eventually results in formation of a fistula in between the gall bladder and the bile duct.
An exception towards the Curvoisier's law.
Complications : Post-cholecystectomy
1) Haemorrhage
Usually the source is from cystic artery.
One should suspect possibility of haemorrhage if the patient complains of persistent abdominal pain, or features of hypovolemic shock during post-operative period
2) Infection
Drastically reduced after administration of prophylactic antibiotics before cholecystectomy.
3) Leakage of bile
Usually due to disrupted ligature, or accidental removal of any accessory ducts.
Patient usually complains of persistent abdominal pain.
If there's no biliary ascites -> ERCP
If there's biliary ascites -> Laparotomy
4) Post-cholecystectomy syndrome
5) Biliary stricture
6) Retained stone
Usually found during T-tube cholangiogram
Any procedure done to explore the common bile duct requires insertion of T-tube.
This is to prevent biliary stasis due to formation of stricture.
The opening of bile duct is sutured to the T-tube, which the long limb is brought out through an abdominal stab incision.
Any bile is collected through a bag.
7-10 days later, T-tube cholangiogram is done (iodine as contrast material)
If there's free flow of contrast material into the duodenum, and there's no residual stone -> remove the T-tube
If there's residual stone :
Stone is small - try using normal saline to irrigate the duct via the T tube (stone eventually migrates to the duodenum)
Stone is large - delayed removal after 4-6 weeks, via radiographically guided removal using dormia basket
Thank you for sharing this good information. Gallstones are believed with the medical establishment to become formed inside your gallbladder. Get you just read a blog write-up about gallstone removal naturally and that is helpful especially those trying to find gallstone remedy. The guide is concerning gallstone removal with apple juice and also I see our people do focus on this too. Begin to see the blog post the following:
ReplyDeletehttp://kidbuxblog.com/removing-gallstones-naturally/
Thanks for sharing this blog, I recently Experience the skill and accuracy of the renowned gall bladder surgeon at the Khosla Stone Kidney & Surgical Centre in Ludhiana. Here Gall bladder surgeon in Ludhianaoffers superior care and direct you toward better health. They have a great deal of experience and knowledge with gallbladder issues.
ReplyDelete