Anatomy of Breast
The vertical extent of breast is from 2nd-6th ribs inclusive.
The horizontal extent is from the lateral edge of sternum to the mid-axillary line.
2/3rds of the breast overlies the pectoralis major muscle, whereas 1/3 of it over the serratus anterior.
The lower medial quadrant is lying on the external oblique aponeurosis, which separates it from the rectus abdominis.
The breast tissue is separated from the pectoralis major muscle by the pectoral fascia. It's anchored anteriorly to the skin, posteriorly to the pectoral fascia by the cooper's ligament.
The outer prolongation of the gland into the axilla at the level of 3rd rib, is known as the axillary tail of spence. It enters the axilla by piercing the opening in the axillary fascia, known as the foramen of langer, and if it's enlarged, it can be mistaken as a lipoma.
The breast tissue is made up of acini, which forms the lobules, and the aggregations of these lobules made up the lobes. Each of these lobes are drained by a collecting duct, and 10-15 of these ducts drains out to the surface of nipple.
If there's a malignant breast lump, infiltrating the cooper's ligament, it'll lead to dimpling of the skin over breast, due to contraction of the cooper's ligament. If the tumour continues to infiltrate along these cooper's ligament, and now involving the pectoral muscle, it renders it lump non-mobile in a direction parallel to the direction of the pectoral muscle fibers, and mobile in a direction perpendicular to it.
If a tumour infiltrates into the major milk ducts, a subsequent fibrosis is going to cause the nipple to be drawn inwards, and hence leading to nipple retraction.
Peu'd orange, an appearance of orange skin of the skin of breast in infiltrative CA breast, is due to the tumour destruction of the cuticle lymphatics, leading to subsequent lymphostasis and edema, and hence the pits of hair follicles appears depressed from the surrounding skin.
Arterial supply
Lateral thoracic artery (major), a branch of the 2nd part of axillary artery
Perforating cutaneous branch of the interal mammary artery to the 2nd, 3rd, 4th space.
Lateral branches of the 2nd, 3rd, 4th intercostal arteries
Venous drainage
Intercostal veins, axillary veins and internal mammary veins
Lymphatic drainage
The primary lymphatic drainage of breast is the axillary nodes (around 20-30 of them), followed by the internal mammary nodes. Around 75% of the lymphatics of the breast is handled by the axillary nodes, and the remaining 25%, by the internal mammary nodes.
There are 5 groups of axillary nodes, namely the anterior, posterior, lateral, central and apical. By surgical means, they can be classified based on their position in relation with the pectoralis minor muscle.
Nodes located below the lateral border the pectoralis minor -> Level I (anterior, posterior and lateral)
Nodes located behind the pectoralis minor muscle -> Level II (central)
Nodes located above the medial border of pectoralis minor muscle -> Level III (apical)
Lymphatics from the lateral quadrant, some from the medial quadrant drains into the anterior nodes (located behind the lower border of pec. major muscle), and the posteior nodes, which then proceeds to the central nodes, and lastly the apical nodes.
Lymphatics from the right axillary and internal mammary nodes drains into the right subclavian lymphatic duct, whilst lymphatics from the left axillary and internal mammary nodes drains into the thoracic duct, then into the subclavian vein. Both eventually drains into the subclavian vein.
Common presenting problem of the breast
1) Painless lump
Breast cancer
Fibroadenoma
An area of fibroadenosis
Breast cyst
2) Painful lump
An area of fibroadenosis
Breast cyst
Periductal mastitis
Breast abscess
Advanced breast carcinoma
3) Only pain
Cyclical mastalgia
Non-cyclical mastalgia
Very rarely, CA breast
4) Nipple changes
Destruction
Depression (retraction, inversion)
Duplication
Discharge
Deviation
Displacement
Remember these 6 Ds
Different causes of nipple discharge :
Fresh red (blood) -> Duct papilloma
Pinkish (blood + serum) -> CA breast
Greenish/Blackish -> Breast cyst
Creamy, pale yellowish -> Duct ectasia
Whitish -> Lactation
Occasionally, paget's disease of the nipple can be confused with eczema of the breast. To differentiate it :
Paget's disease Eczema
Unilateral Bilateral
No vesicles With vesicles
Doesn't itch Itches
May be associated with lump No lump
Nipple may not be intact Nipple is always intact
Post-menopausal Post-lactational
How do you approach in a case of breast lump?
It's by the tripple assessment, which includes history and examination, imaging and Biopsy
1) History
About the lump : Onset, side, site, duration, progression, initial size, current size
Any pain associated with the lump, and proceed to the details of pain
Is there any skin changes? (dimpling, nodules, ulceration, peu'd orange)
Ask about the onset, duration and progression
Is there any nipple discharge?
Ask about the onset, duration, amount, colour, foul-smelling
Is there any recent nipple retraction?
Is there any lumps felt in the axilla?
Then, proceed to the history of risk factors :
Age of menarche (<11 years old)
Age of menopause (>55 years old)
Age of first child birth (if <30 years old, lesser risk)
Parity index (no. of children)
History of breast feeding and the duration (at least 6 months)
Family history of breast cancer (first degree relatives)
HRT/OCP intake (controversial)
Post-menopausal obesity
Diet - Fatty food predilection
Then, h/o of metastases :
Consitutional -> h/o of weight lost, lost of appetite
Respiratory -> Cough, hemoptysis, dyspnoea
CNS -> Headache, vomiting, diplopia, focal neurological deficits, seizures
Liver -> Jaundice
Musculoskeletal -> Bone pain, pathological fractures
2) Examination
a) Comparison of both breasts
Patient is sitting up, both arms are at her side.
Now observe, any discrepency of size and shape of both breasts?
Is there any differences in between the nipples of both sides?
Is there any visible mass?
Now, ask the patient to lift up both of her arms above head
Observe if there's any accentuation of dimpling or distortion of the breasts?
Observe if both breast are elevated equally (if one is higher than the other, it means that the lump probably has fixed to the pec.major muscle)
Now, ask the patient to bend forwards.
Does both breast moves forwards equally?
If one doesn't move as the patient bend forwards, possibly it has fixed to the chest wall (intercostal muscles or ribs)
Now, examine the affected breast.
On inspection, note :
Size and shape - normal?
Skin over breast - peu'd orange, ulcers, nodules, dimpling, dilated veins
Nipple - retraction, discharge
Visible mass - size, shape, surface
Any ulcers - describe it
On palpation, palpate all 4 quadrants of the breast, including the central area and the axillary tail of spence. Note if there's any lump under headings of :
Number of lumps
Site
Size
Surface
Consistency
Tenderness
Edges
Mobility and fixity
First as the patient's hands are placed over her hips, try moving the lump.
If it's not mobile even when the muscles are relaxed, it means that the lump has infiltrated into the chest wall (skin/intercostal muscles).
If it's infiltrated into the serratus anterior, it'll be the same as infiltration to the chest wall, and noted as stage T4 in TMN staging system.
To test whether it has infiltrated to serratus anterior, ask the patient to push against the wall using both hands, and if renders the lump non-mobile, it means infiltration to serratus anterior has taken place.
If the tumour has already infiltrated into the pectoralis major muscle, the lump is mobile in a direction perpendicular to the muscle fibers, but not in a direction parallel to it. This can be confirmed by asking the patient to press firmly using her hands against her hips, and if the lump now is completely immobile, it means infiltration into the pectoralis major muscle has taken place.
Now, try to feel for any lumps of SC nodes.
Examine the axilla, and note any enlarged nodes in it's numbers, consistency, tenderness, fixity.
Percuss the parasternal region for any dullness.
Repeat the same procedure for the opposite breast and axilla.
Now, examine the abdomen -> hepatomegaly, ascites, PR and PV done (metastatic deposits)
Examine the lungs -> Chest wall tenderness, pleural effusions
Check for any bony tenderness
3) Imaging
For women below age of 40 years old, the imaging of choice is ultrasonography
For women above age of 40 years old, imaging of choice is mammography
4) Biopsy
FNAC
TRU-cut/core-needle biopsy
Incisional biopsy
Excisional biopsy
Further test done :
1) Liver function test - elevation of ALP is suggestive of liver metastases
2) Liver ultrasound - liver metastases
3) Chest X ray - pleural effusions, cannon-ball secondaries, rib erosions
4) CT abdomen and Bone scan (optional - not done in MUAR)
TMN staging of CA breast
Tis - Carcinoma in situ
T0 - No evidence of the presence of primary tumour
Tx - Primary tumour cannot be accessed (may be after BCS/mastectomy)
T1 - Size of tumour is < 2cm, not fixed to muslces
T2 - Size of tumour is 2-5cm, fixed to the muscles
T3 - Size of tumour is >5cm
T4a - Involvement of the chest wall
T4b - Involvement of the skin over breast
T4c - Both T4a and T4b present
T4d - Inflammatory carcinoma
N0 - No evidence of nodal metastases clinically
N1 - Ipsilateral axillary nodes palpable, mobile
N2 - Ipsilateral axillary nodes palpable, immobile
N3a - Both infraclavicular and axillary nodes palpable
N3b - Both internal mammary and axillary nodes palpable
N3c - Both axillary and supraclavicular nodes palpable
M0 - No distant metastases
M1 - Distant metastases present
Hence, the stages are :
Stage I - T1 N0 M0
Stage IIA - T0 N1 M0, or T1 N1 M0, or T2 N0 M0
Stage IIB - T2 N1 M0, or T3 N0 M0
Stage IIIA - T0/T1/T2 N2 M0 or T3 N1/N2 M0
Stage IIIB - T4 N0/N1/N2 M0
Stage IIIC - Any T N3 M0
Stage IV - Any T Any N, M1
Wednesday, December 30, 2009
Tuesday, December 29, 2009
Thoracic Trauma
Introduction
Thoracic trauma accounts for about 25% of all cases of trauma.
Most of the thoracic injuries are life theratening, where the commonest cause of morbidity and mortality is hypoxia and haemorrhage.
However, ironically upto 80% of the cases can be managed conservatively.
The key to succesful management here is early physiological resuscitation and accurate diagnosis.
Investigations
An approach towards chest injuries is the same as any other injuries in primary and secondary survey, as noted by the Advanced Trauma Life Support Protocol (ATLS). History and examination will be important, and probably the most useful tool is a chest radiography.
In an unstable patient, chest radiography can be done first, provided that it didn't interfere with the process of resuscitation. An ultrasound can give useful information about the presence of hematoma together with a contusion or just contusion alone. Chest drain can be both diagnostic and therapeutic, where the benefits outweights the risks.
Some pitfalls during investigations :
a) Failed to identify tracheal shift
b) Failed to pass NG tube due to failure to recognise diagphramatic rupture
c) During hemothorax, must auscultate both anterior and posterior chest
d) Failed to resuscitate the patient first before investigations are done (both should be done hand in hand)
Nowadays, CT scan made an important role in the management of chest injuries.
Not only it can provide details about ribs and verterbral fractures, it can pick up contusions, hematomas, pneumothoraces easily. In penetrating injuries, eg gunshot wounds, CT can even trace the track of penetration through the thorax. Though aortogram is the 'gold standard' in diagnosing disruption of thoracic aorta, CT scan yields the similar results.
Immediately life threatening chest injuries :
a) Airway obstruction
The commonest cause of early preventable death in a case of thoracic injury is airway obstruction, which blood, clots, secretions, dentures, teeth or even tongue can be a source of obstruction. Rapid removal usually relieves the obstruction.
Examples of injuries potentially causing airway obstruction :
a) Expanding neck hematomas
b) Bilateral mandibular fractures
Both a and b causing pharyngeal deviation and tracheal compression
c) Laryngeal injury with thyroid/cricoid cartilage fracture, and other tracheal injuries
What need to be done immediately is endotracheal intubation, as early as possible.
Since most of these conditions are insidious and yet progressive, and delay will render increased difficulty in inserting the ET tube.
b) Tension pneumothorax
Tension pneumothorax occurs when "one-way" valve is created in such a way that air is collected within the pleural cavity, without any means of escape. The source of air leakage can be originating from the chest wall or lung parenchyma. This results in significant compression over the affected lung, obstruction of the great veins compromising the venous return, mediastinal shift and eventually, compression of the opposite lung.
Common causes includes, penetrating chest injuries, blunt chest trauma with parenchymal injury, iatrogenic causes includes a central subclavian venepuncture or mechanical positive pressure ventilation that has gone wrong.
The clinical presentation is dramatic, with a panicky patient, complaints of dyspnoea, and with distended neck veins. Clinical signs : Tracheal shift to the opposite side (late presentation), diminished lung expansion over affected side, hyperresonant note on percussion, absence breath sounds.
Tension pneumothorax is a clinical diagnosis, NEVER EVER proceed to radiological investigations first.
If clinical diagnosis is establish, one should use a large bore needle, puncture the anterior chest and the 2nd intercostal space, along the midclavicular line. This is followed by inserting a chest tube over the 5th intercostal space at the anterior axillary line.
c) Pericardial tamponade
In a case of patient with shock and distended vein, pericardial tamponade must be differentiated from tension pneumothorax. Pericardial tamponade is usually caused by penetrating chest injuries, and due to the non-distensible feature of the pericardial sac, even accumulation of small volume of blood is going to cause significant mechanical obstruction which renders cardiac pump failure.
The typical presentation will be : Features of hemorrhagic shock, Raised JVP and CVP, muffled heart sounds. Some pitfalls of these presentation must be remembered :
i) In case where there's active bleeding from a site distant to site of pathology, the neck veins are not distended.
ii) In case where the patient is having circulatory collapse, CVP will not be raised
To buy time for preparing the patient for definite operative management, which is left thoracotomy and sternotomy, a needle pericardiocentesis and resuscitation can be done. Needle pericardiocentesis is NOT a substitute for surgical management, and is done with ECG guidance (related with high incidence of iatrogenic myocardial injury)
d) Open pneumothorax
This means an opening chest wound is present, where the size of the defect is > 3cm.
Every breath that is inhaled, more air will be accumulated within the affected hemithorax.
This eventually causes significant hypoventilation, and eventually hypoxia.
The signs and symptoms are directly proportional to the size of the defect.
Initial management includes covering the chest wound is a sterile plastic occlusive dressing, which is only adhered at 3 sites, creating a flutter-wave valve, while suction is continued, where the tube is connected to an underwater seal drainage bottle.
Remember, no 'sucking' chest wound should be covered completely before a controlled drainage is established..
Definite management : pulmonary debridement and closure of the wound.
Some pit falls regarding this conditions :
For adults, a larger tube is required (>28 FG in size)
Some patients may require 2 chest drains
In case where patient's condition doesn't improve despite adequate drainage, try reducing the pressure within the seal drainage bottle to 5cm H20.
Early mobilisation and physiotherapy is required
e) Massive hemothorax
Defined by : initial blood collection by chest drain of > 1500 ml or in on-going hemorrhage, > 200-300 ml/h of blood collected over a period of 2-3 hours.
Massive hemothorax usually occurs due to blunt injuries, rupturing the intercostal and internal mammary vessels. Blood is hence collected within the affected hemithorax, causing significant respiratory distress. It's recognised by signs of haemorrhagic shock, flat neck veins, diminished expansion, dullness on percussion, absence of breath sounds.
Initial management of massive hemothorax includes chest drain, resuscitation and sometimes, intubation. Blood from the pleural cavity must be drained as rapid and as complete as possible, in order to prevent possibility of empyema and later, fibrothorax.
Pit falls regarding massive hemothorax :
1) One must examine both anterior and posterior chest when the patient is lying in a supine position, since there's a chance where the affected lung 'floats' within the BLOODY thoracic cavity.
If you only auscultate the anterior chest - it'll be normal
2) Even after draining out about 500ml of blood, dullness still persist and radio-opacity still present -> emergency thoracotomy
f) Flial chest
Flial chest is defined as a loss of bony continuity of a chest wall segment with the rest of thoracic cage, caused by a blunt trauma, which occurs when there's :
i) 3 or more rib fractures
ii) occurs in more than 2-3 places
Flial chest is a clinical diagnosis, not by chest radiography.
It's done by observing few respiratory cycles, where the flial segment will be drawn inwards during inspiration.
Causes of hypoxia in flial chest : voluntary splinting due to pain, pulmonary contusion, defect in the mechanical movement of the rib cage
Initial management : opiate analgesics, oxygen support. If a chest drain is present, intrapleural local analgesia can be given. Ventilation is reseved for patients with respiratory failure despite optimal treatment given. Surgical fixation is done in severe thoracic injury or in cases where pulmonary contusion is present.
Thoracic trauma accounts for about 25% of all cases of trauma.
Most of the thoracic injuries are life theratening, where the commonest cause of morbidity and mortality is hypoxia and haemorrhage.
However, ironically upto 80% of the cases can be managed conservatively.
The key to succesful management here is early physiological resuscitation and accurate diagnosis.
Investigations
An approach towards chest injuries is the same as any other injuries in primary and secondary survey, as noted by the Advanced Trauma Life Support Protocol (ATLS). History and examination will be important, and probably the most useful tool is a chest radiography.
In an unstable patient, chest radiography can be done first, provided that it didn't interfere with the process of resuscitation. An ultrasound can give useful information about the presence of hematoma together with a contusion or just contusion alone. Chest drain can be both diagnostic and therapeutic, where the benefits outweights the risks.
Some pitfalls during investigations :
a) Failed to identify tracheal shift
b) Failed to pass NG tube due to failure to recognise diagphramatic rupture
c) During hemothorax, must auscultate both anterior and posterior chest
d) Failed to resuscitate the patient first before investigations are done (both should be done hand in hand)
Nowadays, CT scan made an important role in the management of chest injuries.
Not only it can provide details about ribs and verterbral fractures, it can pick up contusions, hematomas, pneumothoraces easily. In penetrating injuries, eg gunshot wounds, CT can even trace the track of penetration through the thorax. Though aortogram is the 'gold standard' in diagnosing disruption of thoracic aorta, CT scan yields the similar results.
Immediately life threatening chest injuries :
a) Airway obstruction
The commonest cause of early preventable death in a case of thoracic injury is airway obstruction, which blood, clots, secretions, dentures, teeth or even tongue can be a source of obstruction. Rapid removal usually relieves the obstruction.
Examples of injuries potentially causing airway obstruction :
a) Expanding neck hematomas
b) Bilateral mandibular fractures
Both a and b causing pharyngeal deviation and tracheal compression
c) Laryngeal injury with thyroid/cricoid cartilage fracture, and other tracheal injuries
What need to be done immediately is endotracheal intubation, as early as possible.
Since most of these conditions are insidious and yet progressive, and delay will render increased difficulty in inserting the ET tube.
b) Tension pneumothorax
Tension pneumothorax occurs when "one-way" valve is created in such a way that air is collected within the pleural cavity, without any means of escape. The source of air leakage can be originating from the chest wall or lung parenchyma. This results in significant compression over the affected lung, obstruction of the great veins compromising the venous return, mediastinal shift and eventually, compression of the opposite lung.
Common causes includes, penetrating chest injuries, blunt chest trauma with parenchymal injury, iatrogenic causes includes a central subclavian venepuncture or mechanical positive pressure ventilation that has gone wrong.
The clinical presentation is dramatic, with a panicky patient, complaints of dyspnoea, and with distended neck veins. Clinical signs : Tracheal shift to the opposite side (late presentation), diminished lung expansion over affected side, hyperresonant note on percussion, absence breath sounds.
Tension pneumothorax is a clinical diagnosis, NEVER EVER proceed to radiological investigations first.
If clinical diagnosis is establish, one should use a large bore needle, puncture the anterior chest and the 2nd intercostal space, along the midclavicular line. This is followed by inserting a chest tube over the 5th intercostal space at the anterior axillary line.
c) Pericardial tamponade
In a case of patient with shock and distended vein, pericardial tamponade must be differentiated from tension pneumothorax. Pericardial tamponade is usually caused by penetrating chest injuries, and due to the non-distensible feature of the pericardial sac, even accumulation of small volume of blood is going to cause significant mechanical obstruction which renders cardiac pump failure.
The typical presentation will be : Features of hemorrhagic shock, Raised JVP and CVP, muffled heart sounds. Some pitfalls of these presentation must be remembered :
i) In case where there's active bleeding from a site distant to site of pathology, the neck veins are not distended.
ii) In case where the patient is having circulatory collapse, CVP will not be raised
To buy time for preparing the patient for definite operative management, which is left thoracotomy and sternotomy, a needle pericardiocentesis and resuscitation can be done. Needle pericardiocentesis is NOT a substitute for surgical management, and is done with ECG guidance (related with high incidence of iatrogenic myocardial injury)
d) Open pneumothorax
This means an opening chest wound is present, where the size of the defect is > 3cm.
Every breath that is inhaled, more air will be accumulated within the affected hemithorax.
This eventually causes significant hypoventilation, and eventually hypoxia.
The signs and symptoms are directly proportional to the size of the defect.
Initial management includes covering the chest wound is a sterile plastic occlusive dressing, which is only adhered at 3 sites, creating a flutter-wave valve, while suction is continued, where the tube is connected to an underwater seal drainage bottle.
Remember, no 'sucking' chest wound should be covered completely before a controlled drainage is established..
Definite management : pulmonary debridement and closure of the wound.
Some pit falls regarding this conditions :
For adults, a larger tube is required (>28 FG in size)
Some patients may require 2 chest drains
In case where patient's condition doesn't improve despite adequate drainage, try reducing the pressure within the seal drainage bottle to 5cm H20.
Early mobilisation and physiotherapy is required
e) Massive hemothorax
Defined by : initial blood collection by chest drain of > 1500 ml or in on-going hemorrhage, > 200-300 ml/h of blood collected over a period of 2-3 hours.
Massive hemothorax usually occurs due to blunt injuries, rupturing the intercostal and internal mammary vessels. Blood is hence collected within the affected hemithorax, causing significant respiratory distress. It's recognised by signs of haemorrhagic shock, flat neck veins, diminished expansion, dullness on percussion, absence of breath sounds.
Initial management of massive hemothorax includes chest drain, resuscitation and sometimes, intubation. Blood from the pleural cavity must be drained as rapid and as complete as possible, in order to prevent possibility of empyema and later, fibrothorax.
Pit falls regarding massive hemothorax :
1) One must examine both anterior and posterior chest when the patient is lying in a supine position, since there's a chance where the affected lung 'floats' within the BLOODY thoracic cavity.
If you only auscultate the anterior chest - it'll be normal
2) Even after draining out about 500ml of blood, dullness still persist and radio-opacity still present -> emergency thoracotomy
f) Flial chest
Flial chest is defined as a loss of bony continuity of a chest wall segment with the rest of thoracic cage, caused by a blunt trauma, which occurs when there's :
i) 3 or more rib fractures
ii) occurs in more than 2-3 places
Flial chest is a clinical diagnosis, not by chest radiography.
It's done by observing few respiratory cycles, where the flial segment will be drawn inwards during inspiration.
Causes of hypoxia in flial chest : voluntary splinting due to pain, pulmonary contusion, defect in the mechanical movement of the rib cage
Initial management : opiate analgesics, oxygen support. If a chest drain is present, intrapleural local analgesia can be given. Ventilation is reseved for patients with respiratory failure despite optimal treatment given. Surgical fixation is done in severe thoracic injury or in cases where pulmonary contusion is present.
Saturday, December 26, 2009
A case of Acute testicular pain
History

We have a 16 years old male here presented to the ER complaining of sudden onset of right testicular pain. The pain woke him up from his sleep and has persisted over the last 3 hrs. His mother says that he has vomited once. His previous medical history includes a similar event a year ago, but on that occasion the pain subsided quickly. He is an asthmatic and uses a salbutamol inhaler.
Only with h/o, what's your differential diagnosis?
Testicular torsion?
Acute epididymo-orchitis?
Torsion of appendix testis?
Infected hydrocele?
Strangulated hernia?
Testicular rupture?
Haemorrhage into a tumour?
On examination
The left hemi-scrotum feels normal but the right side is acutely swollen and tender on palpation. The testicle is elevated when compared to the other side and has an abnormal horizontal lie. The abdomen is soft, non tender, with intact hernial orifices. Vitals are stable, cremesteric reflex is absent.
So, what's your provisional diagnosis?
In this case, testicular torsion should be ruled out unless proven otherwise. Points towards diagnosis of testicular torsion :
1) Age (testicular torsion is common in age group of 10-25 yrs old)
2) Elevated, tender right testicle
3) Abnormal horizontal lie (risk factor for torsion)
4) Cremesteric reflex is absent (bear in mind that presence of this reflex doesn't rule out testicular torsion!)
If doppler's ultrasound is immediately available, a results showing interrupted blood supply to the testis is diagnostic.
However, if the diagnosis is in doubt, PLS peform surgical exploration to confirm the diagnosis. If not, he CAN SUE YOU BECOZ you've caused him to lose his precious balls.

Remember, you've only 4-6 hours (starting from the time of onset of pain) to salvage the balls.
However, if the patient presented within the first hour after onset of pain, it's sometimes possible to untwist the cord manually, which if succesful, the affected testicle is out of danger and surgery can be planned later.
And, surgical correction is bilateral, since congenital defects often involves both sides.
We have a 16 years old male here presented to the ER complaining of sudden onset of right testicular pain. The pain woke him up from his sleep and has persisted over the last 3 hrs. His mother says that he has vomited once. His previous medical history includes a similar event a year ago, but on that occasion the pain subsided quickly. He is an asthmatic and uses a salbutamol inhaler.
Only with h/o, what's your differential diagnosis?
Testicular torsion?
Acute epididymo-orchitis?
Torsion of appendix testis?
Infected hydrocele?
Strangulated hernia?
Testicular rupture?
Haemorrhage into a tumour?
On examination
The left hemi-scrotum feels normal but the right side is acutely swollen and tender on palpation. The testicle is elevated when compared to the other side and has an abnormal horizontal lie. The abdomen is soft, non tender, with intact hernial orifices. Vitals are stable, cremesteric reflex is absent.
So, what's your provisional diagnosis?
In this case, testicular torsion should be ruled out unless proven otherwise. Points towards diagnosis of testicular torsion :
1) Age (testicular torsion is common in age group of 10-25 yrs old)
2) Elevated, tender right testicle
3) Abnormal horizontal lie (risk factor for torsion)
4) Cremesteric reflex is absent (bear in mind that presence of this reflex doesn't rule out testicular torsion!)
If doppler's ultrasound is immediately available, a results showing interrupted blood supply to the testis is diagnostic.
However, if the diagnosis is in doubt, PLS peform surgical exploration to confirm the diagnosis. If not, he CAN SUE YOU BECOZ you've caused him to lose his precious balls.
Remember, you've only 4-6 hours (starting from the time of onset of pain) to salvage the balls.
However, if the patient presented within the first hour after onset of pain, it's sometimes possible to untwist the cord manually, which if succesful, the affected testicle is out of danger and surgery can be planned later.
And, surgical correction is bilateral, since congenital defects often involves both sides.
Tuesday, December 15, 2009
Head injury - part 3
Management of mild head injury (GCS 14-15)
Most of the occasions, patients with mild head injury, after history and examination, and a period of observation, will be allowed to be discharge after following criterias met :

Battle's sign
a) Full GCS score (15/15)
b) No focal neurological deficits
c) Accompanied by a responsible adult
d) Not under influence of any drugs/alcohol
e) Verbal/Written advice about the injury given

Statement e) means : Advice regarding any worsening of symptoms, such as persistent headahce not relieved by analgesia, severe vomiting, blurring of vision, diplopia, weakness/numbness of limbs have been given verbally or written.
Sometimes, for patients with mild head injury, decision of whether to perform CT brain or not can be a big headahce. However, here are the NICE guidelines regarding indications of CT brain in patients with mild head injury :
a) GCS is <13 at any point
b) GCS is 13-14 at 2 hours time
c) Evidence of focal neurological deficit
d) Suspicion of open, comminuted, depressed, or basal skull fracture
e) Vomiting > 1 episode
f) Seizures
Urgent indication
a) Age > 65 years old
b) Evidence of coagulopathy (liver disease, blood dyscarias, warfarin, anti-platelet medications)
c) Dangerous mechanism of head injury (CT within 8 hrs)
d) Antegrade amnesia > 30 mins (CT within 8 hrs)
Management of moderate/severe head injury
First of all, resuscitation and primary survery.
After stabilising cervical spine at 3 fixation point, start primary surveying.
Remember that normalising the patient's oxygenation and circulation is more important than getting a CT done! This is to prevent secondary brain injury
After primary survey, you've made a diagnosis of moderate/severe head injury, the next step is CT brain, to detect any intracranial hematoma, or any skull fractures, soft tissue injuries, or any mild intracerebral contusion.
For intubated patients, it's recommended that you've asked for CT cervical spine.
Before ariving at the hospital, some conservative management can be given for raised ICP, which includes :
a) Reversed tredelenburg : Raised head upto 20-30 degrees
b) Check if the cervical collar is too tight (may obstruct venous drainage from brain)
c) If there's pupillary dilatation (may be due to acute raised ICP), 0.5mg/kg 20% IV mannitol can be given.
Medical management of severe head injury
Severe head injury is preferably managed in a neurointensive care unit.
ICP can be monitored by passing a catheter into the frontal horn of the lateral ventricle (2 finger breadth from the blurred hole, behind the hairline)
Raise the patient's head for about 20-30 degrees
Protect the patient's airway!
For those with traumatic brain injury and coma, they are more prone to aspiration.
Preferably intubate the patient, and provide high flow oxygen. (Prevent hypoxia)
Make sure that the cervical collar is not too tight.
Cerebral vasculatures are very sensitive to the PCo2 level. When there's a rise in PCo2 level, the cerebral vasculatures dilates, and elevates the ICP. In contrast, when there's a fall in PCo2 level, cerebral vasculature constricts.
Hence, you must try to maintain the PCo2 level in between 4.5-5kPa.
Some experienced anesthetist may induce hyperventilation in patients to cause temporary reduction in ICP by reducing the PCo2 level.
Sedative given, either with or without muscle relaxant.
Mannitol/Frusemide given to reduce cerebral edema.
Patient is prone for hyponatremia or other electrolyte imbalance -> correct it
Avoid pyrexia, as it'll cause undesirable increase in the brain metabolic activity.
Barbiturates eg: thiopentone sodium is given to reduce ICP and brain metabolic rate.
Prophylactic anticonvulsant given.
Most of the occasions, patients with mild head injury, after history and examination, and a period of observation, will be allowed to be discharge after following criterias met :
a) Full GCS score (15/15)
b) No focal neurological deficits
c) Accompanied by a responsible adult
d) Not under influence of any drugs/alcohol
e) Verbal/Written advice about the injury given
Racoon's Sign
Statement e) means : Advice regarding any worsening of symptoms, such as persistent headahce not relieved by analgesia, severe vomiting, blurring of vision, diplopia, weakness/numbness of limbs have been given verbally or written.
Sometimes, for patients with mild head injury, decision of whether to perform CT brain or not can be a big headahce. However, here are the NICE guidelines regarding indications of CT brain in patients with mild head injury :
a) GCS is <13 at any point
b) GCS is 13-14 at 2 hours time
c) Evidence of focal neurological deficit
d) Suspicion of open, comminuted, depressed, or basal skull fracture
e) Vomiting > 1 episode
f) Seizures
Urgent indication
a) Age > 65 years old
b) Evidence of coagulopathy (liver disease, blood dyscarias, warfarin, anti-platelet medications)
c) Dangerous mechanism of head injury (CT within 8 hrs)
d) Antegrade amnesia > 30 mins (CT within 8 hrs)
Management of moderate/severe head injury
First of all, resuscitation and primary survery.
After stabilising cervical spine at 3 fixation point, start primary surveying.
Remember that normalising the patient's oxygenation and circulation is more important than getting a CT done! This is to prevent secondary brain injury
After primary survey, you've made a diagnosis of moderate/severe head injury, the next step is CT brain, to detect any intracranial hematoma, or any skull fractures, soft tissue injuries, or any mild intracerebral contusion.
For intubated patients, it's recommended that you've asked for CT cervical spine.
Before ariving at the hospital, some conservative management can be given for raised ICP, which includes :
a) Reversed tredelenburg : Raised head upto 20-30 degrees
b) Check if the cervical collar is too tight (may obstruct venous drainage from brain)
c) If there's pupillary dilatation (may be due to acute raised ICP), 0.5mg/kg 20% IV mannitol can be given.
Medical management of severe head injury
Severe head injury is preferably managed in a neurointensive care unit.
ICP can be monitored by passing a catheter into the frontal horn of the lateral ventricle (2 finger breadth from the blurred hole, behind the hairline)
Raise the patient's head for about 20-30 degrees
Protect the patient's airway!
For those with traumatic brain injury and coma, they are more prone to aspiration.
Preferably intubate the patient, and provide high flow oxygen. (Prevent hypoxia)
Make sure that the cervical collar is not too tight.
Cerebral vasculatures are very sensitive to the PCo2 level. When there's a rise in PCo2 level, the cerebral vasculatures dilates, and elevates the ICP. In contrast, when there's a fall in PCo2 level, cerebral vasculature constricts.
Hence, you must try to maintain the PCo2 level in between 4.5-5kPa.
Some experienced anesthetist may induce hyperventilation in patients to cause temporary reduction in ICP by reducing the PCo2 level.
Sedative given, either with or without muscle relaxant.
Mannitol/Frusemide given to reduce cerebral edema.
Patient is prone for hyponatremia or other electrolyte imbalance -> correct it
Avoid pyrexia, as it'll cause undesirable increase in the brain metabolic activity.
Barbiturates eg: thiopentone sodium is given to reduce ICP and brain metabolic rate.
Prophylactic anticonvulsant given.
Head Injury - part 2
Extradural hematoma
This refers to collection of blood in between the skull and dura mater.
More commonly seen in younger patients (children, adolescence)
Extradural hematoma is always associated with skull fractures, most frequently, the temporal bone. (since pterion is the thinnest part of skull, involvement of this area causes tearing of the middle meningeal artery)
Of course, involvement of the posterior fossa and frontal bone is also possible.
However, the hematoma is not always arterial in origin, it may be due to a tear to the dural venous sinuses as well.
Classical presentation of extradural hematoma is : (<1/3 of the cases)
Lucid interval, where after initial injury, patient is conscious, alert, oriented, and only complaints of headache. Minutes or hours later, the condition worsens, with deterioration of consciousness, contralateral hemiparesis/plegia, and ipsilateral pupillary dilatation.

Early diagnosis and treatment of subdural hematoma is VITAL.
CT brain is confirmatory, where it'll appears as a lentiform, biconvex, or lense-shaped hyperdense mass in between the skull and brain, with or without midline shift.
After diagnosis is confirmed, surgical evacuation of the hematoma is required, where craniotomy is performed.
Acute subdural hematoma (ASH)

This is actually more common, with poorer prognosis, higher mortality rate as compared to extradural hematoma.
It refers to blood collection in between the dura and arachnoid mater.
ASH is almost always associated with a primary brain injury.
Most of the time at presentation, the patient has impaired consciousness, which rapidly deteriorates depending on the size of the hematoma.

Again, CT brain is diagnostic.
It'll appears as a crescent shaped, more diffuse (with concavity towards the brain), hyperdense mass in between the brain and skull.
Treatment - surgical evacuation by craniotomy
Chronic subdural hematoma (CSH)
CSH often seen in elderly patients, who is on anti-platelets or anti-coagulants. It is believed to be due to tearing of the bridging veins, which causes formation of clinically inapparent, small ASH. Later, as it breaks down and the volume expands, it becomes symptommatic.
Mostly, patients presents with headache, focal neurological deficit, impaired cognition, seizures, etc (hence, one of the d/d of CVA)
CT brain intepretation :
Acute blood (0-10 days) = hyperdense
Subacute blood (10 days - 2 weeks) = isodense
Chronic blood (>2weeks) = hypodense
Treatment = creating a blurr hole and evacuate the hematoma
This refers to collection of blood in between the skull and dura mater.
More commonly seen in younger patients (children, adolescence)
Extradural hematoma is always associated with skull fractures, most frequently, the temporal bone. (since pterion is the thinnest part of skull, involvement of this area causes tearing of the middle meningeal artery)
Of course, involvement of the posterior fossa and frontal bone is also possible.
However, the hematoma is not always arterial in origin, it may be due to a tear to the dural venous sinuses as well.
Classical presentation of extradural hematoma is : (<1/3 of the cases)
Lucid interval, where after initial injury, patient is conscious, alert, oriented, and only complaints of headache. Minutes or hours later, the condition worsens, with deterioration of consciousness, contralateral hemiparesis/plegia, and ipsilateral pupillary dilatation.
Early diagnosis and treatment of subdural hematoma is VITAL.
CT brain is confirmatory, where it'll appears as a lentiform, biconvex, or lense-shaped hyperdense mass in between the skull and brain, with or without midline shift.
After diagnosis is confirmed, surgical evacuation of the hematoma is required, where craniotomy is performed.
Acute subdural hematoma (ASH)
This is actually more common, with poorer prognosis, higher mortality rate as compared to extradural hematoma.
It refers to blood collection in between the dura and arachnoid mater.
ASH is almost always associated with a primary brain injury.
Most of the time at presentation, the patient has impaired consciousness, which rapidly deteriorates depending on the size of the hematoma.
Again, CT brain is diagnostic.
It'll appears as a crescent shaped, more diffuse (with concavity towards the brain), hyperdense mass in between the brain and skull.
Treatment - surgical evacuation by craniotomy
Chronic subdural hematoma (CSH)
CSH often seen in elderly patients, who is on anti-platelets or anti-coagulants. It is believed to be due to tearing of the bridging veins, which causes formation of clinically inapparent, small ASH. Later, as it breaks down and the volume expands, it becomes symptommatic.
Mostly, patients presents with headache, focal neurological deficit, impaired cognition, seizures, etc (hence, one of the d/d of CVA)
CT brain intepretation :
Acute blood (0-10 days) = hyperdense
Subacute blood (10 days - 2 weeks) = isodense
Chronic blood (>2weeks) = hypodense
Treatment = creating a blurr hole and evacuate the hematoma
Monday, December 14, 2009
Head injury - part 1
Pathophysiology
90% of the brain metabolism requires blood-borned glucose.
During normal circumstances, the cerebral autoregulation mechanism maintains the cerebral blood flow above 70mmHg, even though the Mean Arterial Pressure (MAP), varies as much as between 50mmHg - 150 mmHg.
*Cerebral perfusion pressure (CPP) = MAP - ICP
However, when there's head injury, this autoregulatory mechanism is disordered. Hence, the CPP fluctuates with MAP, and hence, brain is more vulnerable towards ischaemia.
According to Monro-Kellie's hypothesis, our skull is a rigid structure, and hence will not expand. Intracranial pressure is directly proportionate to the increase in volume of the intracranial structures, including vascular components (blood in vessels), Cerebrospinal fluid (CSF), or the brain tissue itself.
Initially, when there's formation of a space-occupying lesion, the rise in ICP is prevented by transient displacement of venous blood and CSF away from the brain. This decrease in volume compensates for the rise in volume due to formation of space occupying lesion.
But, further rise in the volume of a brain compartment -> even a slightest increase in volume is going to cause a surge in ICP.
Note : ICP can be measured by passing a catheter through the frontal horn of lateral ventricle. In head injuries, ICP is monitored in btw 5-15 mmHg. Bear in mind that normal ICP is <10mmHg
One should never forget that intracranial hypertension is the dreadliest consequence of head injury. The end-stage of raised ICP will be cerebral herniation, which can be :
a) Herniation through the Tentorial hiatus
Tentorial hiatus is an opening at the tentorium cerebelli
As with central herniation, involving the midbrain, features are :
-> Altered consciousness due to midbrain ischaemia
-> Increased muscle tone, and eventually decorticate rigidity
-> Bilateral +ve babinski's sign
-> pupillary constriction, which followed by dilatation, and lastly, becomes static
As for Lateral herniation, involving the temporal lobe (uncus) :
-> Altered consciousness
-> Contralateral hemiparesis, hemiplegia
-> Compression on the 3rd nerve, initially causing ipsilateral pupillary constriction, followed by dilatation, then becomes fixed to light response. Continued rise in ICP results in involvement of the contralateral side of pupil. The sequence of changes in pupillary response is known as Hutchingson's pupil.
-> Others : ptosis, eye deviated inferolaterally
b) Herniation into foramen magnum
If ICP continues to rise, the cerebellar tonsils will herniates into the foramen of magnum, thereby compressing the brainstem and medulla.
This results in Cardiorespiratory collapse, bilateral pinpoint pupil, and flaccid quadriplegia due to lateral corticospinal tract compression.
Note : Signs of Raised intracranial pressure
Papilloedema (swollen optic disc)
Altered level of consciousness
Bradycardia*
Widened pulse pressure*
Decreased systolic BP*
Abnormal breathing pattern (Cheyne's-Stokes/Hyperventilation)
*Cushing's triad
DO NOT PERFORM LUMBAR PUNCTURE IN A PATIENT WITH RAISED ICP!!
Classification of Head injuries
Classification can be made via :
a) Glasgow Coma scale
Minor head injury = No lost of consciousness and GCS is full 15/15
Mild head injury = GCS 14-15 with lost of consciousness
Moderate head injury = GCS 9-13
Severe head injury = GCS 3-8
b) Mechanism of head injury
i) Blunt trauma
Direct injury (Croup injury)
The brain substance collide against a fixed skull.
Usually caused by sudden deceleration/acceleration forces
Resulting in contusion, laceration and intra-cranial bleeding
Indirect injury (Counter-croup)
Injury to the side opposite to the side of trauma.
Hence, subdural/extradural hematoma may be seen opposite to the side blunt trauma
Rotational injury
This occurs in acceleration/deceleration injury.
Such forces creates rotational injury at the junction btw white/grey matter of brain.
ii) Penetrating injury
High velocity - gunshot injuries
Low velocity - stab injuries
In penetrating injury, there's risk of intracranial infection, due to introduction of foreign bodies
c) Morphological
i) Scalp injuries
Cephalhematoma
More commonly seen in infants and children.
Due to collection of blood under the periosteum, resulting in formation of a tense swelling, confined to the margins of underlying bones.
It takes weeks to resolve
Subaponeurotic hematoma
Blood collection in between aponeurosis and pericranium
Formation of a fluctuant swelling involving the whole scalp
Take weeks to resolve as well
Others : Scalp laceration, Scalding (avulsion)
ii) Skull fractures
It can involve the vault or base, and can be open or closed.
In closed fractures, there's no communication with the exterior, so do not expect a nose, ear bleed or leakage of CSF.
For open vault fractures, expect visible brain substance.
For open base fractures :
If it's an anterior cranial fossa fracture -> Raccoon's Sign (periorbital hematoma) + subconjunctival haemorrhage with no posterior limits + CSF rhinnorhoea and nose bleeding
If it's a middle cranial fossa fracture -> Battle's sign (Bruises seen over mastoid and post-auricular region, which forms within 48 hrs) CSF otorrhoea and ear bleeding
Posterior cranial fossa fracture is not easily identified clinically. Most of the time, when there's occipital bone fracture, there'll be a dural venous sinus tear. Usually, there'll be hypertension, bradycardia, changes in respiration and consciousness.
A closed fracutre can be depressed, communited, or linear.
d) Primary/Secondary
Primary head injury occurs during time of impact, it's irreversible, and not treatable, and recovery will largely depends on the type and extent of injury. Remember that neurons once damaged, will not regenerate.
Hence, most of the our treatment will be focusing on secondary head injury.
Causes of Secondary head injury :
1) Hypoxia, with PaO2 <8Kpa
2) Hypotension, with SBP <90mmHg
3) Cerebral perfusion pressure <65mmHg
4) Intracranial pressure >20 mmHg
5) Pyrexia
6) Seizures
7) Metabolic disturbances
e) Intracranial hematomas
Extradural hematoma
More common in children as their dura strips easily to accomodate blood clot
Here, blood collects between the skull and dura mater
Common at the frontal and temporal region, usually associated with local fractures
Middle meningeal artery or dural venous sinuses are teared
Classical presentation : Lucid interval
Others : Headache, vomiting, lost of consciousness, hemiparesis, seizures, signs of raised ICP
Diagnosis is confirmed by CT brain, which reveals a biconvex, lense-shaped hyperdense hematoma.
If the hematoma is stable, conservative treatment suffice.
However, if there's evidence that it's enlarging, perform blurr hole and craniotomy
Subdural hematoma
More common than extradural hematoma
Here, blood collects between the dura mater and arachnoid mater
Clinical features are similar to extradural hematoma
CT brain reveals a cresent shaped hematoma, which concavity directing towards the brain.
Treatment - same
HISTORY TAKING IN HEAD INJURY
1) How did you injure your head?
Basically, you're asking what's the mechanism of injury.
For dangerous mechanisms, such as falling from a height, or high-speed motor vehicle accident, it may be a multisystem injury, including the spine.
For head injury with lost of consciousness, but without any accidental mechanism, consider hypoglycemia, syncope, aneurysmal subarachnoid haemorrhage
2) Ask about the neurological state of patient during and after injury
Is there lost of consciousness?
Is there seizures?
Is the patient able to respond, move, or talk properly after the injury?
Is there antegrade (can't recall what happened after injury) or retrograde (can't recall what happened before injury) amnesia?
3) Then, What's the GCS of the patient during the scene, prior to intubation, and on arrival in hospital?
4) Is there any evidence suggestive of hypoxia, or any cardiovascular instability?
5) Any co-morbid medical illness?
6) Is the patient taking any drugs? (esp antiplatelets or anticoagulants)
7) Any ilicit drung intake or alcohol consumption
TO BE CONTINUED.....
90% of the brain metabolism requires blood-borned glucose.
During normal circumstances, the cerebral autoregulation mechanism maintains the cerebral blood flow above 70mmHg, even though the Mean Arterial Pressure (MAP), varies as much as between 50mmHg - 150 mmHg.
*Cerebral perfusion pressure (CPP) = MAP - ICP
However, when there's head injury, this autoregulatory mechanism is disordered. Hence, the CPP fluctuates with MAP, and hence, brain is more vulnerable towards ischaemia.
According to Monro-Kellie's hypothesis, our skull is a rigid structure, and hence will not expand. Intracranial pressure is directly proportionate to the increase in volume of the intracranial structures, including vascular components (blood in vessels), Cerebrospinal fluid (CSF), or the brain tissue itself.
Initially, when there's formation of a space-occupying lesion, the rise in ICP is prevented by transient displacement of venous blood and CSF away from the brain. This decrease in volume compensates for the rise in volume due to formation of space occupying lesion.
But, further rise in the volume of a brain compartment -> even a slightest increase in volume is going to cause a surge in ICP.
Note : ICP can be measured by passing a catheter through the frontal horn of lateral ventricle. In head injuries, ICP is monitored in btw 5-15 mmHg. Bear in mind that normal ICP is <10mmHg
One should never forget that intracranial hypertension is the dreadliest consequence of head injury. The end-stage of raised ICP will be cerebral herniation, which can be :
a) Herniation through the Tentorial hiatus
Tentorial hiatus is an opening at the tentorium cerebelli
As with central herniation, involving the midbrain, features are :
-> Altered consciousness due to midbrain ischaemia
-> Increased muscle tone, and eventually decorticate rigidity
-> Bilateral +ve babinski's sign
-> pupillary constriction, which followed by dilatation, and lastly, becomes static
As for Lateral herniation, involving the temporal lobe (uncus) :
-> Altered consciousness
-> Contralateral hemiparesis, hemiplegia
-> Compression on the 3rd nerve, initially causing ipsilateral pupillary constriction, followed by dilatation, then becomes fixed to light response. Continued rise in ICP results in involvement of the contralateral side of pupil. The sequence of changes in pupillary response is known as Hutchingson's pupil.
-> Others : ptosis, eye deviated inferolaterally
b) Herniation into foramen magnum
If ICP continues to rise, the cerebellar tonsils will herniates into the foramen of magnum, thereby compressing the brainstem and medulla.
This results in Cardiorespiratory collapse, bilateral pinpoint pupil, and flaccid quadriplegia due to lateral corticospinal tract compression.
Note : Signs of Raised intracranial pressure
Papilloedema (swollen optic disc)
Altered level of consciousness
Bradycardia*
Widened pulse pressure*
Decreased systolic BP*
Abnormal breathing pattern (Cheyne's-Stokes/Hyperventilation)
*Cushing's triad
DO NOT PERFORM LUMBAR PUNCTURE IN A PATIENT WITH RAISED ICP!!
Classification of Head injuries
Classification can be made via :
a) Glasgow Coma scale
Minor head injury = No lost of consciousness and GCS is full 15/15
Mild head injury = GCS 14-15 with lost of consciousness
Moderate head injury = GCS 9-13
Severe head injury = GCS 3-8
b) Mechanism of head injury
i) Blunt trauma
Direct injury (Croup injury)
The brain substance collide against a fixed skull.
Usually caused by sudden deceleration/acceleration forces
Resulting in contusion, laceration and intra-cranial bleeding
Indirect injury (Counter-croup)
Injury to the side opposite to the side of trauma.
Hence, subdural/extradural hematoma may be seen opposite to the side blunt trauma
Rotational injury
This occurs in acceleration/deceleration injury.
Such forces creates rotational injury at the junction btw white/grey matter of brain.
ii) Penetrating injury
High velocity - gunshot injuries
Low velocity - stab injuries
In penetrating injury, there's risk of intracranial infection, due to introduction of foreign bodies
c) Morphological
i) Scalp injuries
Cephalhematoma
More commonly seen in infants and children.
Due to collection of blood under the periosteum, resulting in formation of a tense swelling, confined to the margins of underlying bones.
It takes weeks to resolve
Subaponeurotic hematoma
Blood collection in between aponeurosis and pericranium
Formation of a fluctuant swelling involving the whole scalp
Take weeks to resolve as well
Others : Scalp laceration, Scalding (avulsion)
ii) Skull fractures
It can involve the vault or base, and can be open or closed.
In closed fractures, there's no communication with the exterior, so do not expect a nose, ear bleed or leakage of CSF.
For open vault fractures, expect visible brain substance.
For open base fractures :
If it's an anterior cranial fossa fracture -> Raccoon's Sign (periorbital hematoma) + subconjunctival haemorrhage with no posterior limits + CSF rhinnorhoea and nose bleeding
If it's a middle cranial fossa fracture -> Battle's sign (Bruises seen over mastoid and post-auricular region, which forms within 48 hrs) CSF otorrhoea and ear bleeding
Posterior cranial fossa fracture is not easily identified clinically. Most of the time, when there's occipital bone fracture, there'll be a dural venous sinus tear. Usually, there'll be hypertension, bradycardia, changes in respiration and consciousness.
A closed fracutre can be depressed, communited, or linear.
d) Primary/Secondary
Primary head injury occurs during time of impact, it's irreversible, and not treatable, and recovery will largely depends on the type and extent of injury. Remember that neurons once damaged, will not regenerate.
Hence, most of the our treatment will be focusing on secondary head injury.
Causes of Secondary head injury :
1) Hypoxia, with PaO2 <8Kpa
2) Hypotension, with SBP <90mmHg
3) Cerebral perfusion pressure <65mmHg
4) Intracranial pressure >20 mmHg
5) Pyrexia
6) Seizures
7) Metabolic disturbances
e) Intracranial hematomas
Extradural hematoma
More common in children as their dura strips easily to accomodate blood clot
Here, blood collects between the skull and dura mater
Common at the frontal and temporal region, usually associated with local fractures
Middle meningeal artery or dural venous sinuses are teared
Classical presentation : Lucid interval
Others : Headache, vomiting, lost of consciousness, hemiparesis, seizures, signs of raised ICP
Diagnosis is confirmed by CT brain, which reveals a biconvex, lense-shaped hyperdense hematoma.
If the hematoma is stable, conservative treatment suffice.
However, if there's evidence that it's enlarging, perform blurr hole and craniotomy
Subdural hematoma
More common than extradural hematoma
Here, blood collects between the dura mater and arachnoid mater
Clinical features are similar to extradural hematoma
CT brain reveals a cresent shaped hematoma, which concavity directing towards the brain.
Treatment - same
HISTORY TAKING IN HEAD INJURY
1) How did you injure your head?
Basically, you're asking what's the mechanism of injury.
For dangerous mechanisms, such as falling from a height, or high-speed motor vehicle accident, it may be a multisystem injury, including the spine.
For head injury with lost of consciousness, but without any accidental mechanism, consider hypoglycemia, syncope, aneurysmal subarachnoid haemorrhage
2) Ask about the neurological state of patient during and after injury
Is there lost of consciousness?
Is there seizures?
Is the patient able to respond, move, or talk properly after the injury?
Is there antegrade (can't recall what happened after injury) or retrograde (can't recall what happened before injury) amnesia?
3) Then, What's the GCS of the patient during the scene, prior to intubation, and on arrival in hospital?
4) Is there any evidence suggestive of hypoxia, or any cardiovascular instability?
5) Any co-morbid medical illness?
6) Is the patient taking any drugs? (esp antiplatelets or anticoagulants)
7) Any ilicit drung intake or alcohol consumption
TO BE CONTINUED.....
Sunday, December 13, 2009
Testicular Tumour
Just breifly describe about this uncommon, but important condition
First, we'll talk about the anatomy :

Testes are originally retroperitoneal organs, during intra-uterine life.
Just before guys are born, our balls descends down, through the inguinal canal, and enters the scrotal sac at the perineum.
As it descends, it bring along vessels, nerves, lymphatics, and it's primary drainage duct - the vas deferens
All these structures are kept safely within the spermatic cord, which can be described of having :

3 vessels : Cremesteric artery, Artery to Vas, and Testicular artery
3 nerves : Autonomic nerves, Genital branch of genitofemoral nerve, and illioinguinal nerve
3 structures : Lymphatics, Pampiniform venous plexus, and Vas deferens
3 coverings : Cremesteric fascia, Internal and external spermatic fascia
The anterior aspect of our testis is covered by a closed peritoneal sac, known as the tunica vaginalis, formed as a result of the obliteration of processus vaginalis.
The posterolateral aspect, is where a single, long coiled duct located, which is the epididymis.
2 histopathological types of Testicular tumour :
1) Seminoma - arising from the seminiferous tubules
2) Teratoma - it's a malignant germ cell tumour
History taking
1) Age
For teratoma, it's common among young men, around 20-30 yrs of age.
Seminoma may be more common in individuals around 30-40 yrs of age.
2) Symptoms
Now, the usual scenario is : the only symptom is a scrotal swelling
Since this condition is usually painless.
Occasionally, there might be some amount of dragging, or dull-aching pain.
Especially when the swelling increases in it's size, the patient might complaints of heaviness over the affected testicles.

In advanced malignancy, there might be symptoms suggesting of metastasis, eg : breathlessness, lost of appetite/weight, abdominal pain, etc
Examination
1) Inspection
A scrotal swelling is seen, not extending into the inguinal region
No expansile cough impulse seen
Scrotal skin - stretched but with normal rugosity, but in advanced stage, skin may ulcerate/infected
No lumps, no scars, no sinuses
2) Palpation
Able to get above the swelling (pure scrotal swelling la)
Testis is enlarged, swollen
Hard in consistency, non tender
There's loss of testicular sensation, and it's feels heavier than the normal side
Spermatic cord is normal
Skin may not be pinchable if infiltration had taken place
Non-fluctuant, non-transilluminant
3) Please examine the para-aortic and supraclavicular lymph nodes
4) Examine the abdomen -> any hepatomegaly? any masses?
Auscultate the lungs -> any signs of metastases?
Investigation
Here I'll try not to be lengthy la har....
1) Blood : Alpha-fetoprotein, B-HCG, and LDH (Tumour markers)
2) Chest X ray (cannon-ball metastases)
3) CT abdomen for staging
4) Orchidectomy and sent specimen for histological analysis
How do we stage it?
Stage I : Only involve the testis
Stage II : Involving the nodes below diagphram
Stage III : Involving the nodes above diagphram
Stage IV : Hepatic/Pulmonary metastasis


So, see how scary it is...
LOVE UR BALLS, MAN!!
First, we'll talk about the anatomy :
Testes are originally retroperitoneal organs, during intra-uterine life.
Just before guys are born, our balls descends down, through the inguinal canal, and enters the scrotal sac at the perineum.
As it descends, it bring along vessels, nerves, lymphatics, and it's primary drainage duct - the vas deferens
All these structures are kept safely within the spermatic cord, which can be described of having :
3 vessels : Cremesteric artery, Artery to Vas, and Testicular artery
3 nerves : Autonomic nerves, Genital branch of genitofemoral nerve, and illioinguinal nerve
3 structures : Lymphatics, Pampiniform venous plexus, and Vas deferens
3 coverings : Cremesteric fascia, Internal and external spermatic fascia
The anterior aspect of our testis is covered by a closed peritoneal sac, known as the tunica vaginalis, formed as a result of the obliteration of processus vaginalis.
The posterolateral aspect, is where a single, long coiled duct located, which is the epididymis.
2 histopathological types of Testicular tumour :
1) Seminoma - arising from the seminiferous tubules
2) Teratoma - it's a malignant germ cell tumour
History taking
1) Age
For teratoma, it's common among young men, around 20-30 yrs of age.
Seminoma may be more common in individuals around 30-40 yrs of age.
2) Symptoms
Now, the usual scenario is : the only symptom is a scrotal swelling
Since this condition is usually painless.
Occasionally, there might be some amount of dragging, or dull-aching pain.
Especially when the swelling increases in it's size, the patient might complaints of heaviness over the affected testicles.
No, It's not painful...
In advanced malignancy, there might be symptoms suggesting of metastasis, eg : breathlessness, lost of appetite/weight, abdominal pain, etc
Examination
1) Inspection
A scrotal swelling is seen, not extending into the inguinal region
No expansile cough impulse seen
Scrotal skin - stretched but with normal rugosity, but in advanced stage, skin may ulcerate/infected
No lumps, no scars, no sinuses
2) Palpation
Able to get above the swelling (pure scrotal swelling la)
Testis is enlarged, swollen
Hard in consistency, non tender
There's loss of testicular sensation, and it's feels heavier than the normal side
Spermatic cord is normal
Skin may not be pinchable if infiltration had taken place
Non-fluctuant, non-transilluminant
3) Please examine the para-aortic and supraclavicular lymph nodes
4) Examine the abdomen -> any hepatomegaly? any masses?
Auscultate the lungs -> any signs of metastases?
Investigation
Here I'll try not to be lengthy la har....
1) Blood : Alpha-fetoprotein, B-HCG, and LDH (Tumour markers)
2) Chest X ray (cannon-ball metastases)
3) CT abdomen for staging
4) Orchidectomy and sent specimen for histological analysis
How do we stage it?
Stage I : Only involve the testis
Stage II : Involving the nodes below diagphram
Stage III : Involving the nodes above diagphram
Stage IV : Hepatic/Pulmonary metastasis


So, see how scary it is...
LOVE UR BALLS, MAN!!
Tuesday, December 8, 2009
History taking and examination of an ulcer
An ulcer is defined as a break in the continuity of the lining epithelium of tissue. Once an ulcer appears, it's usually noticed by the patients, unless it's painless, or located at non-accessible sites.

History taking
1) When do you notice the ulcer?
Remember that the ulcer might have been present for long before the patient actually notices it. This is usually in case of a neuropathic ulcer.
2) What draws your attention to the ulcer?
Usually is because of pain. Others includes : bleeding, discharge, may be foul-smelling.
3) How does the ulcer disturbs you?
The commonest symptom associated with an ulcer is pain. It might be interfering with eating, walking, defecating, etc
4) Any changes to the ulcer since you've noticed it?
Is there any increase in size, changes in shape, increased discharge, bleeding, or severity of pain?
5) Is there any similar ulcers noticed elsewhere in the body?
Asking for multiplicity.
6) What do you think is the cause of ulcer?
Most of the time the patient will get it right, and the commonest cause is trauma.
Examination
1) Inspect the floor
The floor of an ulcer usually made up of granulation tissues or slough tissues. Sometimes, the underlying structures might been exposed, eg : bones, tendons, etc. Some characteristic contents of the floor are able to provide you a hint to your diagnosis :
Solid-Brown, greyish tissue - Full thickness death of tissue
Slough tissue resembles a yellow-grey wash leather - Syphilitic ulcers
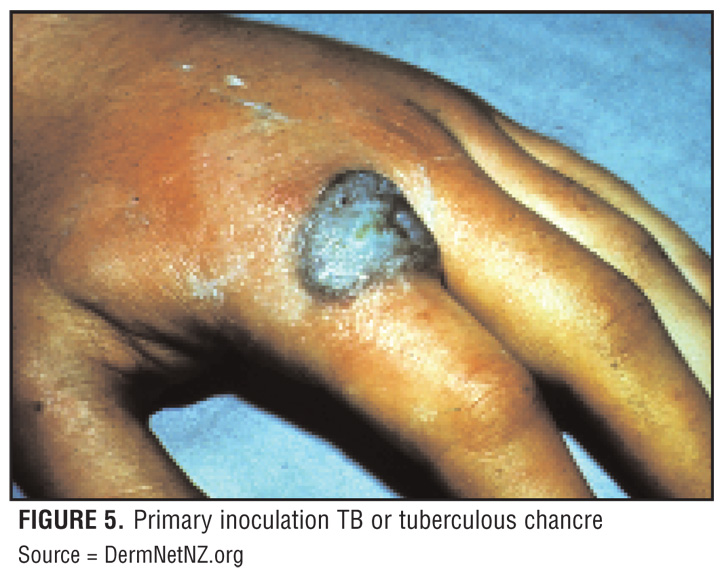
Unhealthy, bluish granulation tissue - Tuberculous ulcers
Poor granulation tissue, with visible bones, tendons, periosteum - Ischaemic ulcer
2) Edge of the ulcer
The edge is the portion in between the floor and margin of an ulcer
There're 5 main types of edges for ulcer :
a) Slopping edge
Usually means the ulcer is superficial/shallow and has a good chance in healing. Healthy granulation tissue usually is pinkish, means it has a good vascularity. A healing epidermis is usually seen extending from the edge, over granulation tissue, either pale/pink in colour (almost transparent)
One example of such ulcer is - venous ulcer

b) Punch-out edge
It means there's rapid death over full thickness of tissue with minimal attempts of the body to repair it. A classical textbook example is the Ulcers seen in tertiary syphilis. Nowadays, ulcers with punch out edges are more commonly seen in neuropathic or peripheral arterial ischaemic ulcers. (PVD)




History taking
1) When do you notice the ulcer?
Remember that the ulcer might have been present for long before the patient actually notices it. This is usually in case of a neuropathic ulcer.
2) What draws your attention to the ulcer?
Usually is because of pain. Others includes : bleeding, discharge, may be foul-smelling.
3) How does the ulcer disturbs you?
The commonest symptom associated with an ulcer is pain. It might be interfering with eating, walking, defecating, etc
4) Any changes to the ulcer since you've noticed it?
Is there any increase in size, changes in shape, increased discharge, bleeding, or severity of pain?
5) Is there any similar ulcers noticed elsewhere in the body?
Asking for multiplicity.
6) What do you think is the cause of ulcer?
Most of the time the patient will get it right, and the commonest cause is trauma.
Examination
1) Inspect the floor
The floor of an ulcer usually made up of granulation tissues or slough tissues. Sometimes, the underlying structures might been exposed, eg : bones, tendons, etc. Some characteristic contents of the floor are able to provide you a hint to your diagnosis :
Solid-Brown, greyish tissue - Full thickness death of tissue
Slough tissue resembles a yellow-grey wash leather - Syphilitic ulcers
Unhealthy, bluish granulation tissue - Tuberculous ulcers
Poor granulation tissue, with visible bones, tendons, periosteum - Ischaemic ulcer
2) Edge of the ulcer
The edge is the portion in between the floor and margin of an ulcer
There're 5 main types of edges for ulcer :
a) Slopping edge
Usually means the ulcer is superficial/shallow and has a good chance in healing. Healthy granulation tissue usually is pinkish, means it has a good vascularity. A healing epidermis is usually seen extending from the edge, over granulation tissue, either pale/pink in colour (almost transparent)
One example of such ulcer is - venous ulcer
It means there's rapid death over full thickness of tissue with minimal attempts of the body to repair it. A classical textbook example is the Ulcers seen in tertiary syphilis. Nowadays, ulcers with punch out edges are more commonly seen in neuropathic or peripheral arterial ischaemic ulcers. (PVD)
c) Undermined edge
It means the rate of destruction of the subcutaneous tissue is more rapid than the skin, causing the edge of ulcer to be undermined. Classical example, as it's rarely seen nowadays is tuberculous ulcers. Ulcers with undermined edge is more commonly seen in bedsores, pressure sores as the subcutaneous tissues are more susceptible towards pressure.
d) Everted edges
This means that over the edges of the ulcer, tissues are growing so rapid that it eventually overlaps the overlying skin. This is classically seen in Squamous cell carcinoma.
e) Rolled edges
The tissues over edges are growing slowly, which is usually pale/pink in colour, with telengiectasis seen over the pearly edges. An ulcer with rolled edges is almost diagnostic of a rodent ulcer of Basal cell carcinoma.
3) Depth
Measure the depth of an ulcer by mm
4) Discharge
Discharge from an ulcer can be serous, serosanginous, sanginous, or purulent.
Sometimes, due to the formation of a coagulation discharge scab over an ulcer, it prevents you from examining the entire structure of ulcer (might be missing some of it's features). It's advised that you remove the scab first.
5) Base
Feel the base of the ulcer.
Is it adherent to the underlying structure? (may be bone, periosteum, tendon in cases of osteomyelitis, malignancy)
6) Regional lymph nodes
Please remember to palpate the regional lymph nodes.
It'll be enlarged (and tender) if there's secondary metastatic deposits or any spreading infection.
7) State of the local tissues
Most of the ulcers over the leg is due to poor vascular/nervous supply.
Hence, it's a must that you check for it's vascularity and innervation.
Monday, December 7, 2009
Advanced Trauma Life Support Protocol (ATLS) - Part 1
In all trauma cases, the 1st hour is also known as the golden hour, since nearly 30% of death occurs during this period of time.

In the ATLS Protocol, it comprises of :
Primary surveilence - Management of immediately life threatening conditions
Secondary surveilence
Definite management
Primary Surveilence
1) Airway
The first thing to do in any trauma cases is to secure the airway.
Stabilise the cervical spine, using the cervical collar. If not possible, place 2 bags of sand over both sides of patient's head serves the same purpose.

Examine the throat, remove any foreign bodies (dentures), blood clots, or suck out any blood/secretions that might be obstructing the airway.
Next, perform jaw thrust on the patient to straighten the airway.
Try inserting the nasopharyngeal/oropharyngeal airway.
If not possible (airway doesn't open up) -> Endotracheal intubation
One of the ways to check whether patient needs intubation is by looking for the gag reflex. If gag reflex is absent -> INTUBATE

Other indications for ET intubation :
1) Hypoxia (PaO2 <70mmHg, PaCO2 >45mmHg)
2) Seizures
3) Deteriorating consciousness
If ET intubation fails, cricothyroidotomy is the next step.
(Easier to perform compared to tracheostomy).
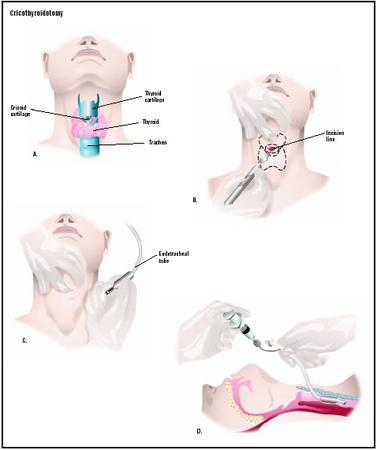
Locate the cricothyroid membrane, apply horizontal stab incision over it using a scapel.
Insert the scapel handle into the surgically created airway, turn it vertically.
Insert a curved tracheostomy tube.
Deliver high flow oxygen (14-15L/min) through nasal prongs, mask or Endotracheal tube.
2) Breathing
Now that you've secure the airway, next is breathing.
On inspection :
Is there stridor? Wheezing?
Count for the respiratory rate.
Is there central cyanosis over the tongue?
Is there usage of accesory muscles of respiration?
Is there obvious wounds over the chest?
Is there any asymmetry in chest movements? (pneumo/hemothorax)
Is there paradoxical chest movements? (flail chest)

On palpation :
Is there tracheal deviation?
Is there any palpable surgical emphysema (palpable crepitation over neck/chest)?
On percussion and auscultation :
Any dull/hyperresonant note on percussion?
Breathing sound -> is it normal on auscultation?
Now, if there's evidence of pneumothorax, hemothorax, next step is to perform chest drain, as below :

1) Prop the patient in semi-reccumbent position
2) Raise the ipsilateral hand above the head
3) Apply incision on the skin over 5th and 6th ribs, at the anterior axillary line
4) Using forceps, dissect (tunneling) the skin until the pleura is visible
5) Puncture the pleura in upwards direction just above the upper border of the ribs. (To avoid neurovascular bundle of intercostal space)
6) Prepare a catheter, with should be clamped first
7) Insert the catheter, place the other end into a underwater drainage seal bottle. Unclamp the cathter
For simple pneumothorax, tube of size 22-24 F is required.
For massive hemothorax/pneumothorax, tube of size 36-40 F is required.
Connect the patient to a pulse oxymeter.
Tension pneumothorax
A medical emergency - any delay -> death ensues
Symptoms -> Dyspnoea, Tachypnoea, Pleuritic chest pain, collapse
Signs -> Hypotension, Raised JVP, Tracheal deviated to opposite, Hyperresonant percussion note, absent breath sounds
Remember that tension pneumothorax is a clinical diagnosis, where immediate decompression is required by means of needle thoracostomy. (Don't waste time during various investigations)

Needle thoracostomy is performed as follows :
1) Use a wide bore needle with catheter, and puncture the 2nd intercostal space on midclavicular line
2) Rapid gush of air indicates tension pneumothorax
3) Remove the needle, insert the catheter
4) Lastly, connect the other end of catheter into a underwater sealed drainage bottle.
3) Circulation
The goal in circulatory assessment is to determine whether the patient is in shock. Signs indicative of shock :
a) Extremities - cool and clammy
b) Prolonged capillary refilling time (normal is <2 secs)
c) Thready/feeble pulse, with rate >100 bpm
d) Hypotension (systolic BP <90 mmHg)
e) Altered mental status - agitation, confusion, unconscious
f) Abnormal respiration
g) Reduced urine output (normal = 1ml/kg/min)
One should immediately gain IV access, using in case signs of shock is present, using short and wide bore cannula of size 14-16 F
Perform fluid resuscitation -> 2L of Crystalloids given (either normal saline/Ringer lactate/Hartmann's solution)
Don't use dextrose!
Dextrose will be metabolised by our body, rendering the fluid hypotonic, and hence unable to maintained within the vascular compartment.
In other words, they are poor plasma expanders
For patients didn't respond to crystalloids, try colloids (gelufundin)
Any revealed/conceal site of hemorrhage -> compression bandage is applied

If patients condition is not improving or there's major bleed, prepare emergency O blood transfusion.
For males, O +ve blood can be given.
However, for females, only O -ve blood can be given for those within reproductive age group.
Now sent blood for investigations :
FBC, Blood grouping/Cross matching, BUSE, Coagulation profile, ABG
Remember to warm the blood before transfusion to prevent hypothermia. Patient should be covered with blankets as well.
If patient's condition is still not improving, use inotropics (either dobutamine, dopamine, adrenaline, nor-adrenaline)
Cardiac tamponade
In cases of hemopericardium, there's compression over the cardiac chambers, causing obstructive shock, where venous return is impeded.
Becks triad of Obstructive shock = Raised JVP, hypotension, faint/absent heart sounds
Can be diagnosed rapidly using FAST (Focused Abdominal Sonography for Trauma)

First, try needle cardiocentesis.
Usually it's unsuccesful since blood within the pericardium is clotted.
Hence, most of the time, surgical decompression is required.
Mean time waiting for surgery, intropics are given.
Detection of bleeding
Stop all revealed hemorrhage - scalp, skin, nose, etc
For other concealed sites, search over the :
Pleural cavity
Peritoneal cavity
Retroperitoneum
Pericardial cavity
Pelvic cavity
Bone fractures
4) Disability
To assess the neurological impairment on patient.
Start with GCS :
Lowest score 3/15, Highest score 15/15
There are 3 components :
Eye movements
Eye opens spontaneously -> 4
Opens only on verbal stimulus -> 3
Opens only on painful stimulus* -> 2
No response -> 1
*given as sternal rub, squeezing of trapezius
Verbal response
Oriented, conversing -> 5
Disoriented, conversing -> 4
Inappropriate words -> 3
Incoherent words -> 2
No response -> 1
Patient is intubated -> T
Motor response
Moves according to instruction -> 6
Localising pain -> 5
Flexion withdrawal -> 4
Abnormal flexion -> 3
Abnormal extension -> 2
No response -> 1
Next, check for pupillary response towards light.
In case of internal hematoma, initially there'll be constriction, followed by dilatation. If ICP is not reduced, the opposite pupil will be affected as well.
Then, identify any signs of raised ICP.
Finally, examine if there's any signs of 3rd, 4th, 6th nerve palsy or any obvious limb paralysis.
5) Exposure
Cut off the clothes to expose other possible wounds (any lacerations, abrasions, contusions)
Inspect the front and back (for the back, perform log roll)
Any fractures -> splint it

Splint/immobilise any swollen/deformed areas, which can be possibly fractured, to prevent further injury, reduce pain and bleeding.
Any compound fracture, sterile dressing should be applied first.
At the end of primary survey, these should be done :
a) Insertion of Ryle's tube

Insert through nostrils -> known as NG tube
If there's nasal bleeding + h/o of head injury -> fracture of skull base
Hence, Ryle's tube is passed through the mouth -> Orogastric tube (OG tube)
b) Urinary catheterization
Using a self-retaining foley's catheter perform a continuous bladder drainage.
If not possible, perform a suprapubic cystostomy.

Bear in mind that any blood present within the urethral meatus, which may indicate urethral rupture, is one of the contraindication against catheterisation.
(You might convert a partial rupture into a complete rupture by passing the tube!)
Other contraindications includes -> pelvic fracture, perineal injury
Monitor urine output -> to be at least 0.5ml/kg/min
c) Wound
Treat any wound by dressing to prevent contamination
Any bleeding wound should be given compressive dressing
d) Monitor
Monitor patient's vital signs (BP, RR, PR, Temperature), GCS, pupillary response, and Oxygen saturation.

For an unstable patient, connect the patient to an ECG monitor and pulse oxymeter.
Monitor patients vital signs every 15 minutes, until the patient is stabilised for more than 1 hour.
e) Investigations
Blood (as mentioned above)
Urine - FEME
X ray
Lateral view of cervical spine
Chest X ray
Pelvic X ray
In the ATLS Protocol, it comprises of :
Primary surveilence - Management of immediately life threatening conditions
Secondary surveilence
Definite management
Primary Surveilence
1) Airway
The first thing to do in any trauma cases is to secure the airway.
Stabilise the cervical spine, using the cervical collar. If not possible, place 2 bags of sand over both sides of patient's head serves the same purpose.
Examine the throat, remove any foreign bodies (dentures), blood clots, or suck out any blood/secretions that might be obstructing the airway.
Next, perform jaw thrust on the patient to straighten the airway.
Try inserting the nasopharyngeal/oropharyngeal airway.
If not possible (airway doesn't open up) -> Endotracheal intubation
One of the ways to check whether patient needs intubation is by looking for the gag reflex. If gag reflex is absent -> INTUBATE
Other indications for ET intubation :
1) Hypoxia (PaO2 <70mmHg, PaCO2 >45mmHg)
2) Seizures
3) Deteriorating consciousness
If ET intubation fails, cricothyroidotomy is the next step.
(Easier to perform compared to tracheostomy).
Locate the cricothyroid membrane, apply horizontal stab incision over it using a scapel.
Insert the scapel handle into the surgically created airway, turn it vertically.
Insert a curved tracheostomy tube.
Deliver high flow oxygen (14-15L/min) through nasal prongs, mask or Endotracheal tube.
2) Breathing
Now that you've secure the airway, next is breathing.
On inspection :
Is there stridor? Wheezing?
Count for the respiratory rate.
Is there central cyanosis over the tongue?
Is there usage of accesory muscles of respiration?
Is there obvious wounds over the chest?
Is there any asymmetry in chest movements? (pneumo/hemothorax)
Is there paradoxical chest movements? (flail chest)

On palpation :
Is there tracheal deviation?
Is there any palpable surgical emphysema (palpable crepitation over neck/chest)?
On percussion and auscultation :
Any dull/hyperresonant note on percussion?
Breathing sound -> is it normal on auscultation?
Now, if there's evidence of pneumothorax, hemothorax, next step is to perform chest drain, as below :
1) Prop the patient in semi-reccumbent position
2) Raise the ipsilateral hand above the head
3) Apply incision on the skin over 5th and 6th ribs, at the anterior axillary line
4) Using forceps, dissect (tunneling) the skin until the pleura is visible
5) Puncture the pleura in upwards direction just above the upper border of the ribs. (To avoid neurovascular bundle of intercostal space)
6) Prepare a catheter, with should be clamped first
7) Insert the catheter, place the other end into a underwater drainage seal bottle. Unclamp the cathter
For simple pneumothorax, tube of size 22-24 F is required.
For massive hemothorax/pneumothorax, tube of size 36-40 F is required.
Connect the patient to a pulse oxymeter.
Tension pneumothorax
A medical emergency - any delay -> death ensues
Symptoms -> Dyspnoea, Tachypnoea, Pleuritic chest pain, collapse
Signs -> Hypotension, Raised JVP, Tracheal deviated to opposite, Hyperresonant percussion note, absent breath sounds
Remember that tension pneumothorax is a clinical diagnosis, where immediate decompression is required by means of needle thoracostomy. (Don't waste time during various investigations)
Needle thoracostomy is performed as follows :
1) Use a wide bore needle with catheter, and puncture the 2nd intercostal space on midclavicular line
2) Rapid gush of air indicates tension pneumothorax
3) Remove the needle, insert the catheter
4) Lastly, connect the other end of catheter into a underwater sealed drainage bottle.
3) Circulation
The goal in circulatory assessment is to determine whether the patient is in shock. Signs indicative of shock :
a) Extremities - cool and clammy
b) Prolonged capillary refilling time (normal is <2 secs)
c) Thready/feeble pulse, with rate >100 bpm
d) Hypotension (systolic BP <90 mmHg)
e) Altered mental status - agitation, confusion, unconscious
f) Abnormal respiration
g) Reduced urine output (normal = 1ml/kg/min)
One should immediately gain IV access, using in case signs of shock is present, using short and wide bore cannula of size 14-16 F
Perform fluid resuscitation -> 2L of Crystalloids given (either normal saline/Ringer lactate/Hartmann's solution)
Don't use dextrose!
Dextrose will be metabolised by our body, rendering the fluid hypotonic, and hence unable to maintained within the vascular compartment.
In other words, they are poor plasma expanders
For patients didn't respond to crystalloids, try colloids (gelufundin)
Any revealed/conceal site of hemorrhage -> compression bandage is applied
If patients condition is not improving or there's major bleed, prepare emergency O blood transfusion.
For males, O +ve blood can be given.
However, for females, only O -ve blood can be given for those within reproductive age group.
Now sent blood for investigations :
FBC, Blood grouping/Cross matching, BUSE, Coagulation profile, ABG
Remember to warm the blood before transfusion to prevent hypothermia. Patient should be covered with blankets as well.
If patient's condition is still not improving, use inotropics (either dobutamine, dopamine, adrenaline, nor-adrenaline)
Cardiac tamponade
In cases of hemopericardium, there's compression over the cardiac chambers, causing obstructive shock, where venous return is impeded.
Becks triad of Obstructive shock = Raised JVP, hypotension, faint/absent heart sounds
Can be diagnosed rapidly using FAST (Focused Abdominal Sonography for Trauma)
First, try needle cardiocentesis.
Usually it's unsuccesful since blood within the pericardium is clotted.
Hence, most of the time, surgical decompression is required.
Mean time waiting for surgery, intropics are given.
Detection of bleeding
Stop all revealed hemorrhage - scalp, skin, nose, etc
For other concealed sites, search over the :
Pleural cavity
Peritoneal cavity
Retroperitoneum
Pericardial cavity
Pelvic cavity
Bone fractures
4) Disability
To assess the neurological impairment on patient.
Start with GCS :
Lowest score 3/15, Highest score 15/15
There are 3 components :
Eye movements
Eye opens spontaneously -> 4
Opens only on verbal stimulus -> 3
Opens only on painful stimulus* -> 2
No response -> 1
*given as sternal rub, squeezing of trapezius
Verbal response
Oriented, conversing -> 5
Disoriented, conversing -> 4
Inappropriate words -> 3
Incoherent words -> 2
No response -> 1
Patient is intubated -> T
Motor response
Moves according to instruction -> 6
Localising pain -> 5
Flexion withdrawal -> 4
Abnormal flexion -> 3
Abnormal extension -> 2
No response -> 1
Next, check for pupillary response towards light.
In case of internal hematoma, initially there'll be constriction, followed by dilatation. If ICP is not reduced, the opposite pupil will be affected as well.
Then, identify any signs of raised ICP.
Finally, examine if there's any signs of 3rd, 4th, 6th nerve palsy or any obvious limb paralysis.
5) Exposure
Cut off the clothes to expose other possible wounds (any lacerations, abrasions, contusions)
Inspect the front and back (for the back, perform log roll)
Any fractures -> splint it
Splint/immobilise any swollen/deformed areas, which can be possibly fractured, to prevent further injury, reduce pain and bleeding.
Any compound fracture, sterile dressing should be applied first.
At the end of primary survey, these should be done :
a) Insertion of Ryle's tube
Insert through nostrils -> known as NG tube
If there's nasal bleeding + h/o of head injury -> fracture of skull base
Hence, Ryle's tube is passed through the mouth -> Orogastric tube (OG tube)
b) Urinary catheterization
Using a self-retaining foley's catheter perform a continuous bladder drainage.
If not possible, perform a suprapubic cystostomy.
Bear in mind that any blood present within the urethral meatus, which may indicate urethral rupture, is one of the contraindication against catheterisation.
(You might convert a partial rupture into a complete rupture by passing the tube!)
Other contraindications includes -> pelvic fracture, perineal injury
Monitor urine output -> to be at least 0.5ml/kg/min
c) Wound
Treat any wound by dressing to prevent contamination
Any bleeding wound should be given compressive dressing
d) Monitor
Monitor patient's vital signs (BP, RR, PR, Temperature), GCS, pupillary response, and Oxygen saturation.
For an unstable patient, connect the patient to an ECG monitor and pulse oxymeter.
Monitor patients vital signs every 15 minutes, until the patient is stabilised for more than 1 hour.
e) Investigations
Blood (as mentioned above)
Urine - FEME
X ray
Lateral view of cervical spine
Chest X ray
Pelvic X ray
Sunday, December 6, 2009
OGDS and Colonoscopy
As Housemen, you need to know about the indications, preparations, complications
Oesophagogastroduodenoscopy (OGDS)

Indications :
1) For investigation of :
Dyspepsia
Upper GI symptoms not responsive to optimal treatment
Patients >45 yrs with alarmic dyspeptic symptoms, eg :
Chest pain
Odynophagia
Weight loss
Anemia, evidence of GI bleeding
Dysphagia
Dysphagia/Odynophagia
Unexplained iron deficiency anemia
GI bleeding (Acute/Recent/Occult)
Re-evaluation of previous upper GI bleeding
Confirmation of radiologically demonstrated lesion
Suspected portal hypertension
Surveillance of tissue/fluid sampling (Barrett's/Polyposis)
2) Therapeutic interventions
On-going upper GI bleeding (variceal for eg)
Variceal treatment
Removal of selected polyps
Removal of foreign bodies
Dilatation of stenotic lesions
Placement of feeding tube
Palliative treatment for neoplasm
Preparation :
1) Informed consent
2) Patient may need to stop anti-platelet medications (aspirin, clopidogrel) 1 week prior to procedure, and diabetic medication 1 day before procedure
3) Antibiotic prophylaxis for patients with :
Undergoing high-risk endoscopies : Dilatation of stenotic lesions, Variceal bleeding
Previous h/o of infective endocarditis, those with prosthetic heart valves
4) Nil by mouth at least 6 hours prior to procedure
5) Pre-procedural investigations :
FBC, Blood grouping/Cross matching, Coagulation profile, UPT, urinalysis, ECG and chest X ray
6) Sedative given before procedure (diazepam). Hence, ask patient not to come alone or don't drive after procedure.
Contraindications :
Uncooperative patients, Medically unstable patients, risk of perforation is high
Complications : Bleeding, infection, perforation, cardiopulmonary problems
Colonoscopy

Removal of foreign bodies
Treatment of bleeding
Excision of polyps
Decompression/Megacolon/Volvulus
Preparations :
1) Informed consent
2) Patient may need to stop anti-platelet medications (aspirin, clopidogrel) 1 week prior to procedure, and diabetic medication 1 day before procedure
3) Antibiotic prophylaxis for patients with previous h/o of infective endocarditis, those with prosthetic heart valves
4) 2 days prior to procedure, avoid solid foods, take only food which are easily digestible, eg :
Porridge, Noodles in clear soup, Low Fibre food
5) 1 day prior to procedure, only fluids !
eg, Coffee/Tea without milk, Carbonated drinks (not reddish/purplish), Strained fruit juices
6) Laxatives taken 1 day prior to procedure (tablets bisacodyl)
7) Night before procedure - NIL BY MOUTH
8) Day of procedure - try to empty bowel before procedure
9) Sedative given.
Oesophagogastroduodenoscopy (OGDS)
Indications :
1) For investigation of :
Dyspepsia
Upper GI symptoms not responsive to optimal treatment
Patients >45 yrs with alarmic dyspeptic symptoms, eg :
Chest pain
Odynophagia
Weight loss
Anemia, evidence of GI bleeding
Dysphagia
Dysphagia/Odynophagia
Unexplained iron deficiency anemia
GI bleeding (Acute/Recent/Occult)
Re-evaluation of previous upper GI bleeding
Confirmation of radiologically demonstrated lesion
Suspected portal hypertension
Surveillance of tissue/fluid sampling (Barrett's/Polyposis)
2) Therapeutic interventions
On-going upper GI bleeding (variceal for eg)
Variceal treatment
Removal of selected polyps
Removal of foreign bodies
Dilatation of stenotic lesions
Placement of feeding tube
Palliative treatment for neoplasm
Preparation :
1) Informed consent
2) Patient may need to stop anti-platelet medications (aspirin, clopidogrel) 1 week prior to procedure, and diabetic medication 1 day before procedure
3) Antibiotic prophylaxis for patients with :
Undergoing high-risk endoscopies : Dilatation of stenotic lesions, Variceal bleeding
Previous h/o of infective endocarditis, those with prosthetic heart valves
4) Nil by mouth at least 6 hours prior to procedure
5) Pre-procedural investigations :
FBC, Blood grouping/Cross matching, Coagulation profile, UPT, urinalysis, ECG and chest X ray
6) Sedative given before procedure (diazepam). Hence, ask patient not to come alone or don't drive after procedure.
Contraindications :
Uncooperative patients, Medically unstable patients, risk of perforation is high
Complications : Bleeding, infection, perforation, cardiopulmonary problems
Colonoscopy
Indications :
1) Investigation
Unexplained iron deficiency anemia
Altered bowel habits
Chronic diarrhoea
Inflammatory bowel disease
Lower GI bleeding for patients >40 yrs of age (occult blood is included)
2) Therapeutic
Treatment of bleeding
Excision of polyps
Decompression/Megacolon/Volvulus
Preparations :
1) Informed consent
2) Patient may need to stop anti-platelet medications (aspirin, clopidogrel) 1 week prior to procedure, and diabetic medication 1 day before procedure
3) Antibiotic prophylaxis for patients with previous h/o of infective endocarditis, those with prosthetic heart valves
4) 2 days prior to procedure, avoid solid foods, take only food which are easily digestible, eg :
Porridge, Noodles in clear soup, Low Fibre food
5) 1 day prior to procedure, only fluids !
eg, Coffee/Tea without milk, Carbonated drinks (not reddish/purplish), Strained fruit juices
6) Laxatives taken 1 day prior to procedure (tablets bisacodyl)
7) Night before procedure - NIL BY MOUTH
8) Day of procedure - try to empty bowel before procedure
9) Sedative given.
Scrotal swelling
Classifications
1) Congenital

Congenital hydrocele
Congenital indirect inguinal hernia
2) Inflammatory
Cellulitis of scrotal skin - skin appears red, shinny, warm, tender
Pyocele - pus accumulation within tunica vaginalis, fluctuates, non-transilluminant

Orchitis/Epididymo-orchitis/Epididymitis - tender, non-fluctuent swelling
Funiculitis - tender and thickened spermatic cord
3) Neoplastic
There's no benign testicular tumours!
Malignant
Primary : Seminoma, Teratoma, Leydig cell tumour, Sertoli cell tumour, Lymphoma
Secondaries from other sites
4) Others
Hydrocele
Hydatid cyst of morgagni
Epididymal cyst (smooth, uni/multi-locular swelling located behind the testis, brilliantly transilluminate)

Spermatocele (above and behind the upper pole of testis, poorly transilluminate)
Encysted hydrocele of the cord
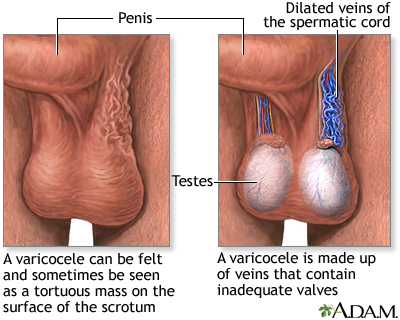
Varicocele
History taking
1) Onset
Sudden onset of scrotal swelling may be hematocele (with h/o of trauma)
Acute onset can be inflammatory causes (Epididymitis, Orchitis, E-Orchitis)
Insidious - usually hydrocele or testicular tumour
2) Progression
Rapid progression - inflammatory swellings or hemorrhage into a cyst/hydrocele
3) Association with pain
Inflammatory swellings are painful.
Acute epididymo-orchitis must be differentiated from Testicular torsion.

The former, as testis is elevated - pain reduces (increases support on testis)
The latter, as testis is elevated - pain worsens (increases the degree of torsion)
4) Association with fever
Low, moderate, high grade
Intermittent, remittent, continuous
Both acute epididymo-orchitis and scrotal abscess presents with fever
5) Urinary symptoms
A positive h/o of UTI is important for acute epididymo-orchitis
Ask for frequency and dysuria
On examination
1) Inspection
Comment whether one side or both sides are involved
Check whether the swelling extends up to the inguinal region, which can be :
Infantile hydrocele
Inguino-scrotal hernia
Ask the patient to cough, look for expansile cough impulse, which can be :
Hernia, Congenital hydrocele
Inspect the skin over swelling, comment on it's colour and rugosity, whether :
Stretched + shinny -> inflammatory
Stretched + normal rugosity -> Hydrocele, testicular tumours
Inspect whether there's any skin lumps.
Any scars, sinuses?
2) Palpation
Try to get above the swelling, it means that the cord is palpable above the swelling. This is to confirm that it's a pure scrotal swelling.
Comment on the position of testis :
Swelling is anterior to testis -> Hydrocele (but usually hydrocele will be too large for the testis to be separately palpable)
Swelling is attached to the top of testis, cystic -> Hydatid cyst of morgagni
Cystic swelling behind the testis, more towards the upper pole -> Epididymal cyst
Swelling above and behind the upper pole of testis -> Spermatocele
Cystic swelling palpable at the root of scrotum -> Encysted hydrocele of cord
(Can be mistaken as direct inguinal hernia - try pulling the scrotal skin down, it'll descend and becomes less mobile)
Testicular swellings can be either tumour or inflammatory
Varicocele - feels like a bag of worms
Tenderness - for any inflammatory swellings (acute pyocele, hematocele, acute epididymo-orchitis), and sometimes, very tensed cyst
Consistency
Soft - Spermatocele
Cystic - Epididymal cyst
Tense - Hydrocele
Firm - Acute epididymo-orchitis
Hard - Testicular tumours
Palpate the contents of scrotum
Feel for the cord and vas deferens.
The vas deferens will be normal but the cord is thickened - testicular tumour
Both vas deferens and cord is thickened and tender - Acute epididymo-orchitis
Skin not pinchable - testicular tumours infiltrated to skin
Varicocele - bag of worms while patient standing, resolves as he lies down
Cough impulse - Felt in case of hernia, palpable thrill in varicocele
Fluctuation positive - all swelling contains fluid

Transillumination test
3) Examine the inguinal nodes
4) Examine the abdomen
1) Congenital
Congenital hydrocele
Congenital indirect inguinal hernia
2) Inflammatory
Cellulitis of scrotal skin - skin appears red, shinny, warm, tender
Pyocele - pus accumulation within tunica vaginalis, fluctuates, non-transilluminant
Orchitis/Epididymo-orchitis/Epididymitis - tender, non-fluctuent swelling
Funiculitis - tender and thickened spermatic cord
3) Neoplastic
There's no benign testicular tumours!
Malignant
Primary : Seminoma, Teratoma, Leydig cell tumour, Sertoli cell tumour, Lymphoma
Secondaries from other sites
4) Others
Hydrocele
Hydatid cyst of morgagni
Epididymal cyst (smooth, uni/multi-locular swelling located behind the testis, brilliantly transilluminate)
Spermatocele (above and behind the upper pole of testis, poorly transilluminate)
Encysted hydrocele of the cord
Varicocele
History taking
1) Onset
Sudden onset of scrotal swelling may be hematocele (with h/o of trauma)
Acute onset can be inflammatory causes (Epididymitis, Orchitis, E-Orchitis)
Insidious - usually hydrocele or testicular tumour
2) Progression
Rapid progression - inflammatory swellings or hemorrhage into a cyst/hydrocele
3) Association with pain
Inflammatory swellings are painful.
Acute epididymo-orchitis must be differentiated from Testicular torsion.
The former, as testis is elevated - pain reduces (increases support on testis)
The latter, as testis is elevated - pain worsens (increases the degree of torsion)
4) Association with fever
Low, moderate, high grade
Intermittent, remittent, continuous
Both acute epididymo-orchitis and scrotal abscess presents with fever
5) Urinary symptoms
A positive h/o of UTI is important for acute epididymo-orchitis
Ask for frequency and dysuria
On examination
1) Inspection
Comment whether one side or both sides are involved
Check whether the swelling extends up to the inguinal region, which can be :
Infantile hydrocele
Inguino-scrotal hernia
Ask the patient to cough, look for expansile cough impulse, which can be :
Hernia, Congenital hydrocele
Inspect the skin over swelling, comment on it's colour and rugosity, whether :
Stretched + shinny -> inflammatory
Stretched + normal rugosity -> Hydrocele, testicular tumours
Inspect whether there's any skin lumps.
Any scars, sinuses?
2) Palpation
Try to get above the swelling, it means that the cord is palpable above the swelling. This is to confirm that it's a pure scrotal swelling.
Comment on the position of testis :
Swelling is anterior to testis -> Hydrocele (but usually hydrocele will be too large for the testis to be separately palpable)
Swelling is attached to the top of testis, cystic -> Hydatid cyst of morgagni
Cystic swelling behind the testis, more towards the upper pole -> Epididymal cyst
Swelling above and behind the upper pole of testis -> Spermatocele
Cystic swelling palpable at the root of scrotum -> Encysted hydrocele of cord
(Can be mistaken as direct inguinal hernia - try pulling the scrotal skin down, it'll descend and becomes less mobile)
Testicular swellings can be either tumour or inflammatory
Varicocele - feels like a bag of worms
Tenderness - for any inflammatory swellings (acute pyocele, hematocele, acute epididymo-orchitis), and sometimes, very tensed cyst
Consistency
Soft - Spermatocele
Cystic - Epididymal cyst
Tense - Hydrocele
Firm - Acute epididymo-orchitis
Hard - Testicular tumours
Palpate the contents of scrotum
Feel for the cord and vas deferens.
The vas deferens will be normal but the cord is thickened - testicular tumour
Both vas deferens and cord is thickened and tender - Acute epididymo-orchitis
Skin not pinchable - testicular tumours infiltrated to skin
Varicocele - bag of worms while patient standing, resolves as he lies down
Cough impulse - Felt in case of hernia, palpable thrill in varicocele
Fluctuation positive - all swelling contains fluid
Transillumination test
3) Examine the inguinal nodes
4) Examine the abdomen
Common Anal Diseases
Briefly about anatomy of anal canal






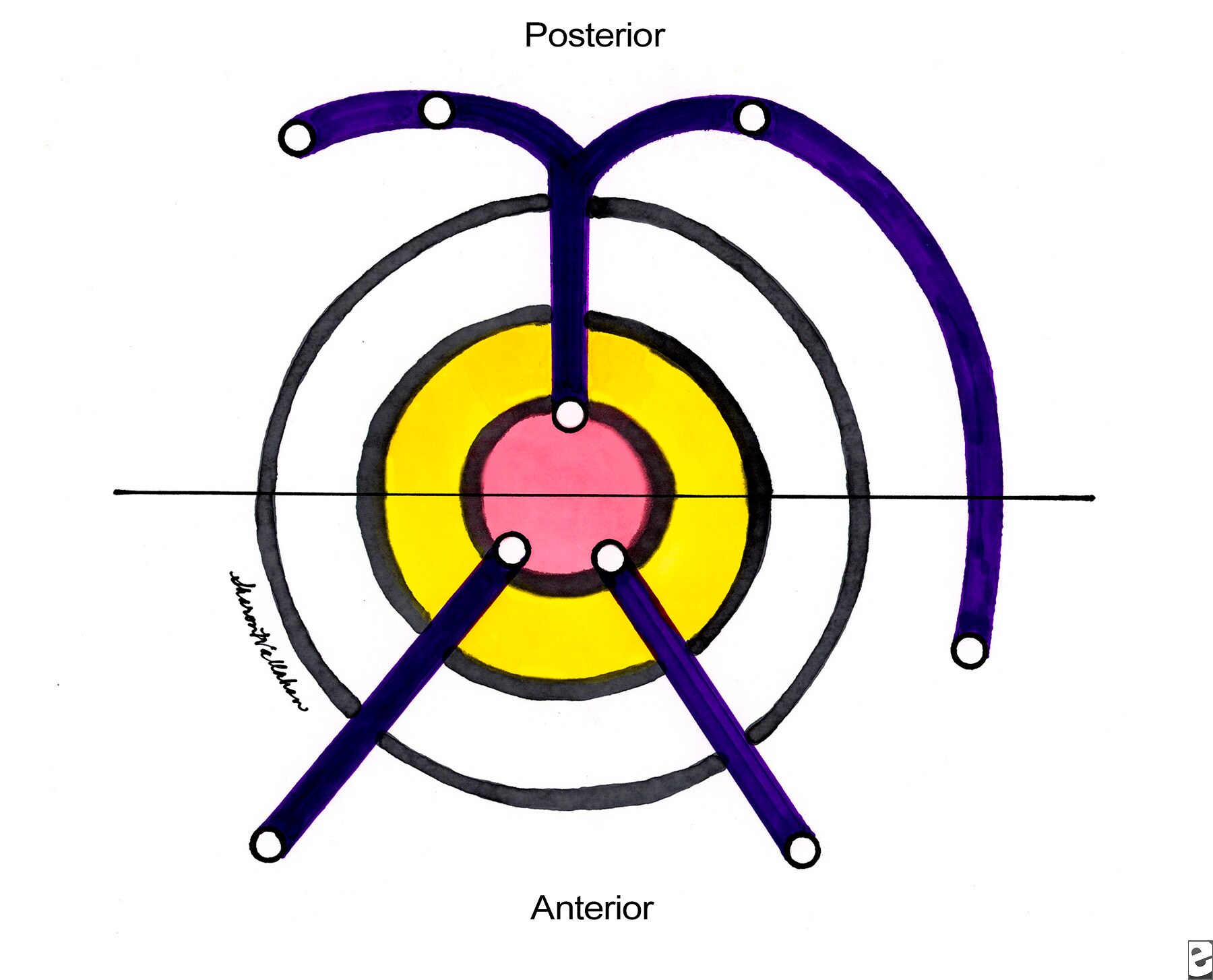

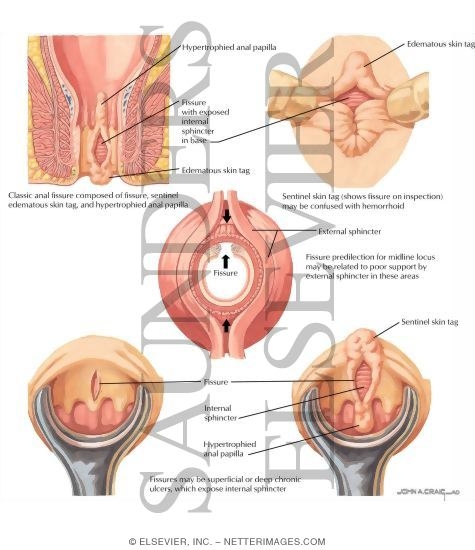

The anal canal commences from the level where the rectum passes through the pelvic diaphragm towards the anal verge. The junction in between the anal canal and rectum is the anorectal ring/bundle which can be felt during PR examination.
The internal sphinchter is a circular, non-striated, involuntary muscles innervated by autonomic nerves.
The external sphincter is striated, voluntary muscles innervated by pudendal nerves.
The superior part of external sphincter fuses with the puborectalis muscle to form the anorectal bundle, for maintainance of continence.
The lower part of anal canal is lined by the sensitive squamous cell epithelium
The lymphatic drainage of the lower half of anal canal is drained into the inguinal lymph nodes
Blood supply - superior, middle and inferior rectal vessels.
Haemorrhoids
The anal canal contains 3 anal cushions, which serves as a gas-fluid protective barrier and closes it. When these cushions enlarge, they can prolapse, and when they're damaged, it causes bleeding.
Chronic hemorrhoids produces pile mass, as the processes are compressing on the perianal skin below it, produces external skin tags.
How it cause bleeding?
As these vascular pads becomes haemorrhoids, they assumed into a position closer to the anorectal junction.
During defecation, as the anal canal everts, the stools compressed against the vascular pads, scratching the mucosa over it.
After defecation, the vascular pads are remained scratched, and hence, blood start to trickle down.
If the vascular pads are unable to reduce after the anal sphincter closes, it worsens the bleeding by impairing it's venous return.
Symptoms (History)
Usually seen in individuals > 20 yrs of age. Extremely rare in children.
Bear in mind that uncomplicated piles are not painful.
Hence, it usually causing painless PR bleeding, which can be mild (notice on wiping your ASS after shitting), or can be severe to the extent of splashing all over the lavatory and eventually causing iron deficiency anemia.
Due to mucus discharge from the surface of hemorrhoids, it can cause pruritus ani.
Another important symptom is sensation of prolapse after defecation, or palpable lump. This forms the basis of the classification of piles based on the severity of prolapse :
Grade 1 : Only bleeding, no prolapse
Grade 2 : Prolapse occurs, but reduces spontaneously
Grade 3 : Doesn't reduce spontaneously (reduce manually)
Grade 4 : Irreducible
However, such classification is artificial, since every hemorrhoids prolapsed during defecation, the only way where it leads to bleeding.
Hence, to translate it clinically :
Grade 1
Prolapse occurs during defecation, but reduces back to it's normal position when the anal sphincter closes. Hence, no lump is noticed by the patient.
Grade 2
The prolapse occured during defecation, reduces back spontaneously but slowly.
Only complicated piles, when it strangulates, thrombosed, becomes gangrenous, fibrosed causing pain. Also known as acute hemorrhoidal crisis.
If the patient has any underlying coagulopathy, bleeding disorders, or taking aniticoagulants, piles may bleed massively.
Examination
Don't ever forget that non-prolapsed/thrombosed piles can't be diagnosed by your fingers! It's indistinguishable from normal mucosa.
Hence, a sigmoidoscopy/proctoscopy is very much required.
However, 3rd/4th degree hemorrhoids, since it's visible, you may be able to make a spot diagnosis.
It's a bluish-purplish swelling, with diameter of 1-2cm, with soft mucosal surface, usually non-tender (unless complicated), with mucus-exuding surface.
If it's complicated, it'll be tense, tender, oedematous.
Sigmoidoscopy and proctoscopy is still required to rule out other rectal pathology.
Management
For acute hemorrhoidal crisis, many surgeons thought that surgical intervention at this stage may cause portal pyemia.
But, it's not true -> if early antibiotic coverage is given.
Yet, many surgeons usually wait until the acute phase is over, and then only decide whether hemorrhoidectomy is required.
During acute phase :
Analgesics given.
Apply cold/warm saline bag pressure -> mass usually shrinks after 3-4 days
For 1st-2nd degree haemorrhoids :
Give defecatory advice - only shit when the desire is there (don't simply shit), apply correct shitting position to minimise straining, in addition of stool softerners and bulk forming agents.
Not responsive -> Submucosal injection of 5% phenol in almond oil
Indications of hemorrhoidectomy
1) 3rd-4th degree
2) 2nd degree non-responsive to non-operative management
3) Fibrosed haemorrhoids
Perianal hematoma
It's actually a misnomer, since it's not a true hematoma.
It's caused by thrombosis of a subcutaneous veins within the anal tissue, secondary to injury of venous wall while straining on defecation.
The thrombosis subsequently causing inflammation and edema of the surrounding tissues.
History
Age
Any age, no sexual predilection
Symptoms
Characterised by anal pain, which gradually increases in it's intensity over hours, and subsides after a few days. It causes a continuous discomfort, worsened by sitting, walking, etc.
It is associated with the presence of a lump in the anus, which initially small in size, and gradually enlarges when it becomes more painful.
If the lump ruptures through the skin, or it ulcerates, it can cause PR bleeding.
Since it causes partial opening of the anus, as there's continuous mucus discharge, it results in pruritus ani.
Can be triggered by episodes of straining at stools while defecating.
Signs
The lump can be located anywhere along the anal margin.
The skin over it appears reddish-purplish.
Size is usually small initially (1x1cm), with hemispherical shape, gradually enlarges in size, which becomes polypoidal.
With smooth surface, hard in consistency.
It's tender, but disproportionate to what the patient complaints of.
Not fix to the skin, nor it can be reduced back into the anal canal.
Local/regional lymph nodes are not enlarged.
Fistula in ano
A fistula is a track, lined by squamous epithelium/granulation tissues, connecting two epithelised surface, either in between 2 body cavities, or 1 body cavity - external skin surface.
Hence, fistula in ano is an abnormal, fistulous connection between the rectum or anal canal to the external skin. Usually caused by a ruptured intersphincteric abscess. It has an external opening on the skin, and an internal opening, which can be classified based on it's relative position to the anorectal ring :
High level fistula
Internal opening located above the anorectal ring. As it tracks through the anorectal bundle, it causes incontinence. Different varieties of it includes :
Extra-sphincteric, Trans-sphincteric, Inter-sphincteric
Low level fistula
Internal opening located below anorectal ring. It doesn't cause incontinence.
Different varieties includes :
Trans-sphincteric, Inter-sphincteric, Subcutaneous/Submucosal
Goodsall's rule
According to goodsall's rule, any anterior fistula will have it's internal opening located along a line drawn radially, connecting the external opening to the anus.
Whilst any posterior fistula, regardless of it's position, will have is internal opening, located at the posteior anus, on midline position.
History
Patient may have h/o of perianal abscess, might have been drained or healed.
Commonest symptoms is watery, serous, purulent discharge from the external opening.
They may complaint of bubbling sensation during defecation, as stool passes through the anal canal, it forces mucous discharge from the fistula. This also prevents healing of the fistula.
Periodic throbbing pain can be there as pus accumulates within the tract.
Persistent mucous discharge causing pruritus ani.
Some amount of bleeding might be there. (from external opening)
In your history taking, also ask for symptoms of inflammatory bowel disease, any abdominal upset, systemic upset.
On examination
You'll notice that the discharge can be either serous or pustulous.
The external opening is seen as tufts of granulation tissues or puckered scars.
Rectal examination is usually not painful.
The internal opening is felt as an area of induration or a nodule under the anal mucosa. Most of the time, the tract is palpable.
Look for any other evidence of Anal carcinoma, TB, or IBD.
Confirm your examination findings using sigmoidoscopy/proctoscopy.
If the inguinal nodes are enlarged -> either due to infection of the fistulous tract, or infiltrative anal carcinoma.
Treatment : Fistulotomy, Fistulectomy
Anal fissure
Defined as a longituidinal split in the anal skin.

Acute tear is common, especially when there's excessive straining during defecation (hard stools?), and it usually heals rapidly. But during next defecation, as the stool stretches the anal canal, it causes the split to gape, leading to pain and bleeding. Then, it's so painful that the anal sphincter undergoes spasm.
Hence, a viscious cycle of tear-pain-spasm occurs, and produces further pain. Eventually, as the fissure becomes chronic, fibrosis occurs and a chronic ulcer is produced.
History
This condition can be quite common in children as they frequently passes bulky stools rapidly.
In adults, usually occurs in between 20-40 yrs of age, slightly more common in males. In females, might be seen after delivery.
Severe anal pain on defecation is the chief complaint, which is tearing in character. Persistent, throbbing pain is there minutes or even hours after defecation. It's sometimes so painful that the patient might be apprehensive towards defecation, and ended up accumulating large volume of hard stools within the rectum. This only causes more pain during next defecation.
Since there's spasm of anal sphincter, patient might find it difficult to pass motion. (As for laymen, constipation)
There's streaking of stools with blood, or the patient notices blood while wiping their ass after defecation. As with chronic fissure, there's only mild-bleeding.
In chronic fissures, sometimes there's a sentinel-skin tag palpable at the lower end of the fissure. And due to the hypertrophy of the anal papillae, mucus discharge from the ulcer causing pruritus ani.
Examination
Most anal fissures are located at the posterior midline of anal skin, some at the anterior midline, rarely lateral.
Usually diagnosed by separating the anal skin, and the split is visible.
Rectal examination is usually not possible as it's too painful.
However, if it's not too painful for the patient, anal skin defect can be felt during examination, surrounded by area of induration.
NO proctoscopy/sigmoidoscopy should be done on a conscious patient !!!
Subscribe to:
Posts (Atom)