Decided to stop posting in Madicine@ and Surgicomania.
Notice that there's not much of HO in East Malaysia who blogs.
Many medical students or potential ones may be curious about life as a HO in Sabah and Sarawak.
Starting another blog. Days of my life....
Thanks for the comments in the clinical cases that I've posted.
Didn't know that there's actually someone out there who knew the existence of this blog.
Friday, September 30, 2011
Monday, August 23, 2010
Briefly about Pancreatic Pseudocyst
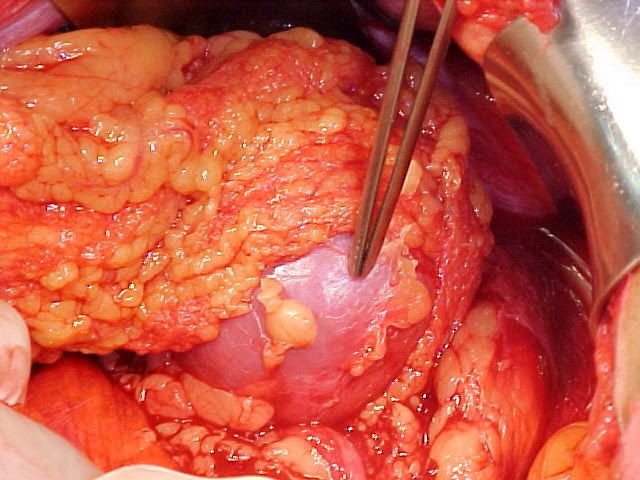
Pancreatic pseudocyst is defined as single/multiple fluid collection with high amylase content, surrounded by fibrous or granulation tissue within the lesser sac.

It usually occurs around 4 weeks after an acute attack of pancreatitis, where patient complains of epigastric fullness, pain, nausea and vomiting.
If it's infected, there may be fever, rigors and sweating.
However, pseudocyst can be also caused by chronic pancreatitis or any pancreatic trauma.
Abdominal examination
Firm, tender epigastric mass is felt, with indistinct lower edge, and inability to get above the swelling.
It moves slightly with respiration.
Percussion reveals resonant note since the pseudocyst is covered by stomach.
However, it's not possible to demonstrate fluctuation and fluid thrill.
Investigations
Pancreatic pseudocyst must be differentiated from acute fluid collection and pancreatic abscess.
Usually just based on the clinical scenario and USG abdomen (or sometimes CT), one will be able to distinguish these conditions.
However, one must not forget that a cystic neoplasm may mimic as a chronic pseudocyst.
To differentiate, one needs to perform aspiration of the swelling under EUS guidance (EUS = endoscopic ultrasound).
Then, sent the aspirate for amylase level, cytology and CEA level.
Typically, if it's a chronic pseudocyst - high amylase level, with leucocytes and CEA < 400 ng/ml.
However, in case of mucinous neoplasm - CEA > 400 ng/ml.
Complications

Treatment
Treatment consist of drainage of the pseudocyst.
There are 3 approaches towards the drainage :
1) Percutaneous transgastric cystogastrostomy under imaging guidance, then by placing a double pigtail catheter, one end within the cystic cavity, another within the gastric lumen for drainage.
Chance of recurrence : not more than 15 %

2) Endoscopic method under EUS guidance : By puncturing the wall of stomach/duodenum to gain access into the pseudocyst cavity, then insertion of a drainage tube one end within the cystic cavity, another within the gastric lumen for drainage.
3) Surgical method by internal drainage into gastric/jejunal lumen. Rate of recurrence is not more than 5%.
It usually occurs around 4 weeks after an acute attack of pancreatitis, where patient complains of epigastric fullness, pain, nausea and vomiting.
If it's infected, there may be fever, rigors and sweating.
However, pseudocyst can be also caused by chronic pancreatitis or any pancreatic trauma.
Abdominal examination
Firm, tender epigastric mass is felt, with indistinct lower edge, and inability to get above the swelling.
It moves slightly with respiration.
Percussion reveals resonant note since the pseudocyst is covered by stomach.
However, it's not possible to demonstrate fluctuation and fluid thrill.
Investigations
Pancreatic pseudocyst must be differentiated from acute fluid collection and pancreatic abscess.
Usually just based on the clinical scenario and USG abdomen (or sometimes CT), one will be able to distinguish these conditions.
However, one must not forget that a cystic neoplasm may mimic as a chronic pseudocyst.
To differentiate, one needs to perform aspiration of the swelling under EUS guidance (EUS = endoscopic ultrasound).
Then, sent the aspirate for amylase level, cytology and CEA level.
Typically, if it's a chronic pseudocyst - high amylase level, with leucocytes and CEA < 400 ng/ml.
However, in case of mucinous neoplasm - CEA > 400 ng/ml.
Complications

Treatment
Treatment consist of drainage of the pseudocyst.
There are 3 approaches towards the drainage :
1) Percutaneous transgastric cystogastrostomy under imaging guidance, then by placing a double pigtail catheter, one end within the cystic cavity, another within the gastric lumen for drainage.
Chance of recurrence : not more than 15 %
2) Endoscopic method under EUS guidance : By puncturing the wall of stomach/duodenum to gain access into the pseudocyst cavity, then insertion of a drainage tube one end within the cystic cavity, another within the gastric lumen for drainage.
3) Surgical method by internal drainage into gastric/jejunal lumen. Rate of recurrence is not more than 5%.
Wednesday, July 21, 2010
Colonic diverticular disease
Introduction
Colonic diverticular disease is very common in developed nations, which is related to their diet containing low dietary fibers.
It is estimated that in developed countries, there are about 60% of the population aged > 70 years old are affected by diverticular disease. But this condition is rare before 35 years old.
Incidence is more common among females.

Though the entire colon may be affected, but the commonest site is the sigmoid colon, probably after intake of low residual diet, the intramural pressure over sigmoid colon is the highest.
Pulsion of diverticulae emerged in between the mesenteric and anti-mesenteric taenia, through the circular muscles, at points where the blood vessels penetrates through it.
Hence, diverticular disease will never occur in the rectum.
This is due to it's different arrangement of blood vessel, and it's longitudinal smooth muscle covers the entire circumference of the rectum.
Sometimes, a caecal diverticula may be obstructed by a faecolith or by inflammatory processes.
Hence resulting in acute appendicitis (mimics simple acute appendicitis)
Clinical features
Colonic diverticular disease are mostly asymptommatic.
Most of the cases are detected during investigation of other GI diseases, where diverticular disease are found incidentally.
Occasionally, patient may present with intermittent lower abdominal/LIF pain and tenderness.
Other symptoms include minor rectal bleeding, defecation urgency, altered bowel habits, etc.

Barium enema shows intestinal smooth muscular hypertrophy with multiple diverticula.
Complications
1) Perforation
Purulent peritonitis
Fecal peritonitis
2) Inflammation
Pericolic abscess

Peridiverticulitis
3) Fistula formation
Colovaginal
Colovesical
Colocolonic
Colocutaneous
4) Intestinal obstruction
Colonic fibrous fistula
Inflammatory mass, fistula
Adherent loops of small bowel
5) Bleeding
Chronic intermittent bleeding
Massive lower GI bleeding
Acute diverticulitis
1) History
Initially, patient may complains of intermittent lower abdominal pain.
Later, the pain is shifted to the left iliac fossa, which gradually becomes more constant, dull aching in nature.
If there's intestinal obstruction, the pain can be colicky in nature as well.
Often, there is lost of appetite, and nausea (rarely vomiting).
If the colonic vault is close to the bladder, it is not uncommon for the patient to have bladder symptoms (frequency, dysuria)
2) On examination
Patient appears in obvious distress, with fever and tachycardia.
Over the left iliac fossa, there is significant tenderness and guarding.
Occasionally, a tender, sausage-shaped mass may be palpable over the left iliac fossa.
Reverse Rovsing's sign is +ve : RIF is pressed, and pain is felt over LIF.
If there's intestinal obstruction or generalised peritonitis, abdomen is distended, with rebound tenderness, while on auscultation, bowel sounds is hyperactive (obstruction), or reduced (paralytic ileus - peritonitis).

Acute diverticulitis can be confirmed by Barium enema.
However, it is better to have it done 4-6 weeks later after infection has subsided.
Management
Nil by mouth
Bed rest
IV fluids
Antibiotics (Cephalosporins, Metronidazole)
If doesn't resolve, suspect pericolic abscess formation.
May requires incision and drainage of abscess, surgical resection, peritoneal toilet.
Colonic diverticular disease is very common in developed nations, which is related to their diet containing low dietary fibers.
It is estimated that in developed countries, there are about 60% of the population aged > 70 years old are affected by diverticular disease. But this condition is rare before 35 years old.
Incidence is more common among females.
Though the entire colon may be affected, but the commonest site is the sigmoid colon, probably after intake of low residual diet, the intramural pressure over sigmoid colon is the highest.
Pulsion of diverticulae emerged in between the mesenteric and anti-mesenteric taenia, through the circular muscles, at points where the blood vessels penetrates through it.
Hence, diverticular disease will never occur in the rectum.
This is due to it's different arrangement of blood vessel, and it's longitudinal smooth muscle covers the entire circumference of the rectum.
Sometimes, a caecal diverticula may be obstructed by a faecolith or by inflammatory processes.
Hence resulting in acute appendicitis (mimics simple acute appendicitis)
Clinical features
Colonic diverticular disease are mostly asymptommatic.
Most of the cases are detected during investigation of other GI diseases, where diverticular disease are found incidentally.
Occasionally, patient may present with intermittent lower abdominal/LIF pain and tenderness.
Other symptoms include minor rectal bleeding, defecation urgency, altered bowel habits, etc.
Barium enema shows intestinal smooth muscular hypertrophy with multiple diverticula.
Complications
1) Perforation
Purulent peritonitis
Fecal peritonitis
2) Inflammation
Pericolic abscess
Peridiverticulitis
3) Fistula formation
Colovaginal
Colovesical
Colocolonic
Colocutaneous
4) Intestinal obstruction
Colonic fibrous fistula
Inflammatory mass, fistula
Adherent loops of small bowel
5) Bleeding
Chronic intermittent bleeding
Massive lower GI bleeding
Acute diverticulitis
1) History
Initially, patient may complains of intermittent lower abdominal pain.
Later, the pain is shifted to the left iliac fossa, which gradually becomes more constant, dull aching in nature.
If there's intestinal obstruction, the pain can be colicky in nature as well.
Often, there is lost of appetite, and nausea (rarely vomiting).
If the colonic vault is close to the bladder, it is not uncommon for the patient to have bladder symptoms (frequency, dysuria)
2) On examination
Patient appears in obvious distress, with fever and tachycardia.
Over the left iliac fossa, there is significant tenderness and guarding.
Occasionally, a tender, sausage-shaped mass may be palpable over the left iliac fossa.
Reverse Rovsing's sign is +ve : RIF is pressed, and pain is felt over LIF.
If there's intestinal obstruction or generalised peritonitis, abdomen is distended, with rebound tenderness, while on auscultation, bowel sounds is hyperactive (obstruction), or reduced (paralytic ileus - peritonitis).
Acute diverticulitis can be confirmed by Barium enema.
However, it is better to have it done 4-6 weeks later after infection has subsided.
Management
Nil by mouth
Bed rest
IV fluids
Antibiotics (Cephalosporins, Metronidazole)
If doesn't resolve, suspect pericolic abscess formation.
May requires incision and drainage of abscess, surgical resection, peritoneal toilet.
Friday, May 7, 2010
Acute Pancreatitis and CA pancreas
Introduction

Defined as activation of the pancreatic enzyme resulting in autolysis of the gland.
It is important to investigate for the possible causes of Acute pancreatitis before labeling it as 'idiopathic'.
Possible aetiology of Acute pancreatitis :
Gall stones
Alcoholism
Post ERCP
Abdominal trauma
Complication of cardiothoracic, biliary and abdominal surgery
Hypercalcemia
Hyperparathyroidism
Pancreatic Divisum
Autoimmune pancreatitis
Scorpion bite
Drugs : Corticosteroids, Azathioprine, Thiazide diuretics
Mumps, Cocksakie viral infection
Idiopathic
History
Both males and females are equally affected.
Age of onset is around 4th - 5th decade of life.
History of any gall stone diseases, or alcoholism is important (2 most important cause)
Though rare, but ask for recent contact with children with mumps or cocksakie infection.
Symptoms are usually triggered after consumption of large meal or alcohol.
Patient usually complains of sudden onset of severe, continuous epigastric pain, which typically radiates to the back, relieved by bending forwards.
It's accompanied by excessive vomiting and retching, with persistent nausea in between.
Breathing and movements exacerbates the pain.
General examination
Patient appears ill, with shallow breathing.
If the patient looks pale, diaphoretic, it is likely that it has complicated as a hypovolemic shock.
There might be mildly tinged jaundice if the pancreatitis is caused by gall stones.
Even 2-3 days after the illness, the mild tinged jaundice can be caused by compression of biliary duct by edematous head of pancreas.
Shock features of tachycardia, hypotension.
Low grade fever may or may not present.
Abdominal examination
In acute pancreatitis, the complains of the patient may indicate severe pain, but there is usually minimal findings
during abdominal examination.
 Cullen's sign
Cullen's sign
 Grey Turner's sign
Grey Turner's sign
On inspection, if there's haemorrhagic pancreatits, there might be bruising (bluish purplish) discolouration over around the umbilicus (Cullen's sign) or left flank (Grey Turner's sign).
However, these signs are rarely seen nowadays.
The abdomen may not rise and fall with respiration, since the musculature is tightly contracted, and during onset of paralytic ileus.
Often there is accumulation of inflammatory exudates within the lesser sac, which eventually forms pseudocyst, suggested by epigastric fullness (distension), dullness during percussion over it.
Shifting dullness may be present, bowel sound may be reduced if there is pancreatic ascites.
Invesitgations
Acute pancreatitis is usually diagnosed by typical clinical presentation and laboratory investigation that reveals elevated serum amylase level. Serum amylase of 3-4 times greater than the normal level is suggestive of pancreatitis.
However, if serum lipase assay is available, it is more sensitive and specific.
Note that normal serum amylase level doesn't rule out Acute pancreatitis, and the level poorly correlates with the severity.
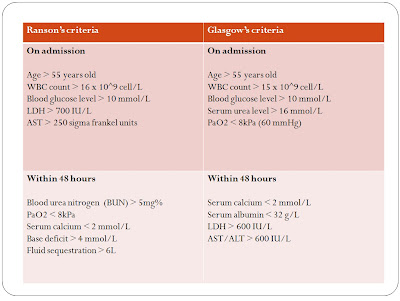
Both Ranson's and Glasgow's criteria is used to grade the severity of Acute pancreatitis.
If 3 or more factors are present in the patient, it indicates severe pancreatitis.
 Imaging studies
Imaging studies
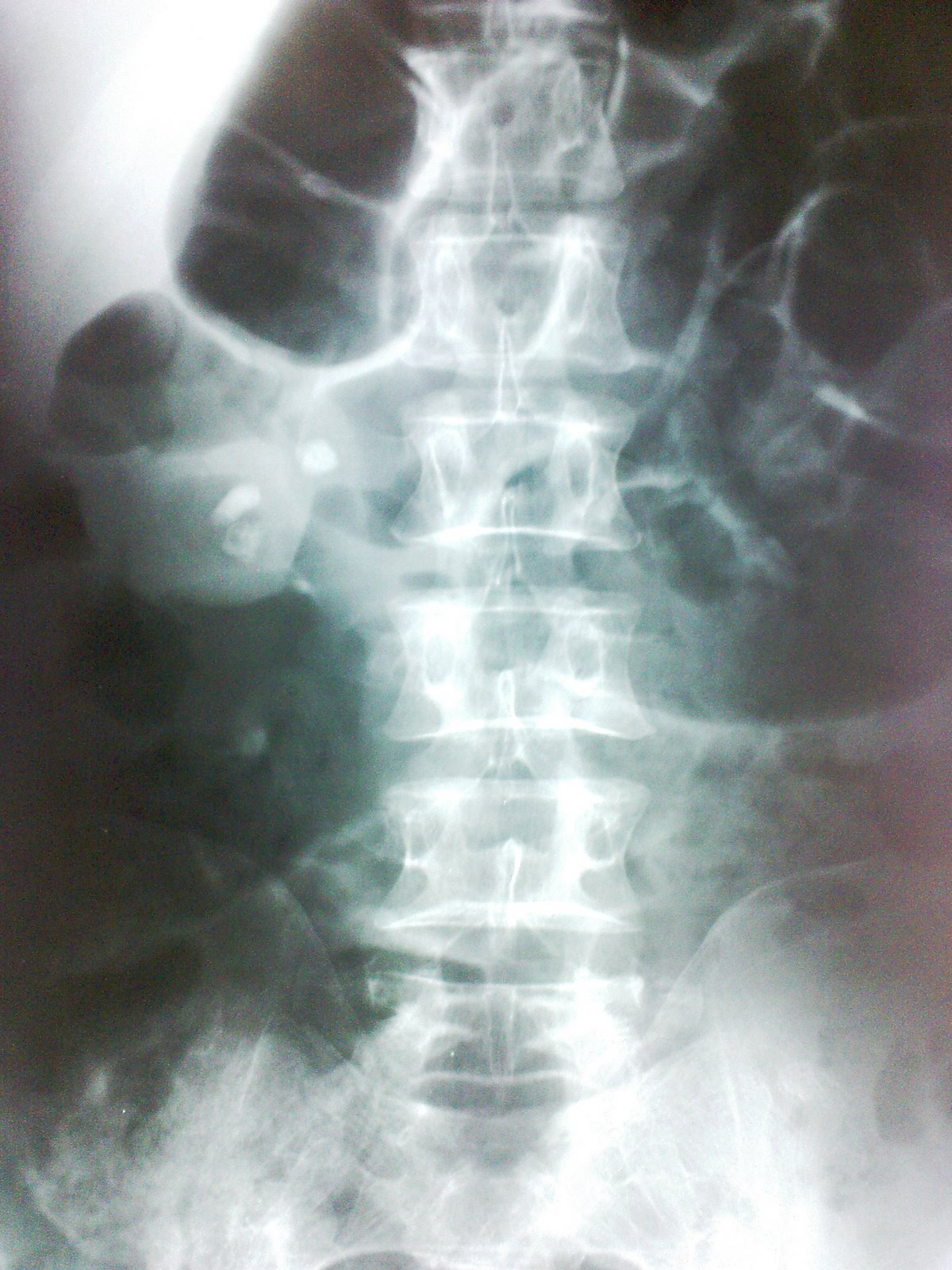
Chest X ray, and plain abdominal X ray is not very helpful in the diagnosis of Acute pancreatitis
During early stages, if abdominal X ray is taken, non-specific signs such as Sentinel loop, Renal Halo sign or Colon cut off sign may be present.
 Sentinel loop
Sentinel loop
 Colon cut-off sign
Colon cut-off sign
Chest X ray may reveal pleural effusion, or if there is diffuse alveolar infiltrates, indicates ARDS.
Though Abdominal USG is non-diagnostic for Acute pancreatitis, but it must be done within 24 hours of presentation.
This is to rule out Acute cholecystitis as a differential diagnosis, to check whether the bile duct is dilated and to reveal any stones within the CBD (gall stone as a cause of Pancreatitis)
CT abdomen is not indicated in every patient.
Only when :
1) Diagnostic uncertainty
2) Severe pancreatitis
3) Clinical deterioration, with multi-organ failure, sepsis
4) Local complications occurs
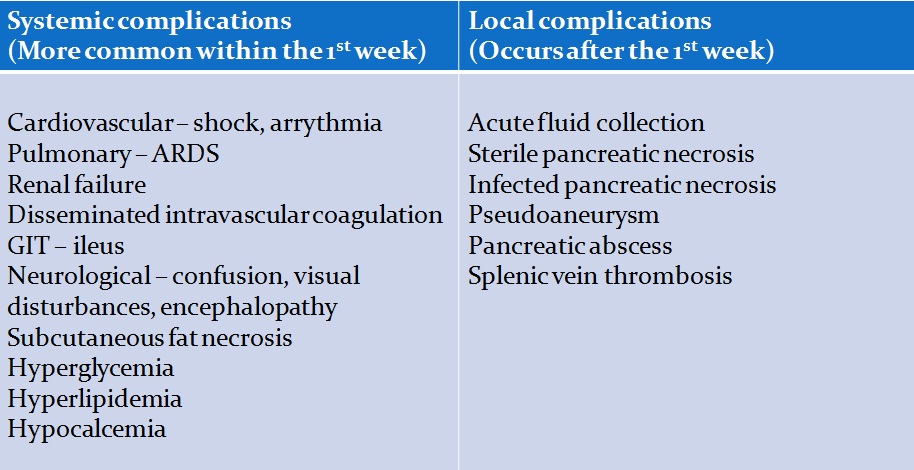
Complications
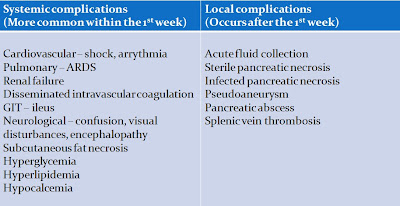
Pancreatic pseudocyst
Management
a) Conservative
1) Gain IV access and rapid fluid resuscitation.
2) Give analgesics (usually IM pethidine is given)
3) Nil by mouth
4) Insertion of NG tube to relieve vomiting
5) Enteral feeding - nasojejunal tube (to maintain adequate nutrition)
6) Urinary catheterization is done
7) Monitor pulse, BP, urine output and CVP
8) Give antibiotics to prevent secondary infection
b) Endoscopic
If gall stone is strongly suspected as the cause of pancreatitis, the stones should be removed by basket (dormia) through endoscopic sphincterotomy.
If there is severe pancreatitis, or cholangitis occurs, both sphinterotomy and ERCP is done.
c) Surgery
Only indicated if : clinical deterioration during conservative management, unsure diagnosis, local complication occurs.
Adenocarcinoma of Pancreas
More common in males.
Age of presentation - 55-75 years old
85% of CA pancreas involves the head of pancreas, where the prognosis is usually poor.
Patients usually dies within 1 year of diagnosis (5 year survival is exceptional)
Upon presentation, most have progressed to a surgically incurable stage.
Though uncommon, but tumour arising from the distal CBD, duodenum and ampulla has a better outlook.
Currently, the risk factor of developing CA pancreas is thought to be :
Cigarette smoking
High fat and protein diet
Clinical features
Any elderly patient presents with painless jaundice, always suspect the possibility of Pancreatic cancer.
Typical symptoms are usually : Abdominal pain, jaundice and weight loss.
Jaundice is usually obstructive in nature, suggested by the classical triad of pruritus, clay-coloured stool and tea-coloured urine.
There might be steatorrhoea.
Abdominal pain - constant, dull aching, discomfort, over the epigastric region
Sought for symptoms of metastases
On examination, the gall bladder may be palpable, as accordance to the Curviosier's law, which states that,
"For patients presenting with clinically evident jaundice, and on examination the gall bladder is palpable, the cause is more likely to be due to Carcinoma of the Head of Pancreas".
Look for scleral icterus, hepatomegaly, etc.
Investigations
If stool occult blood test is positive, suggestive of a ampullary tumour.
Abdominal USG - usually done to look for liver metastases, or any mass lesion over the pancreas, and dilated bile ducts
CT abdomen - extent of metastases
To confirm the nature of obstruction, MRCP is preferred over ERCP since the former is less invasive.
Surgery of choice : Whipple's procedure

Defined as activation of the pancreatic enzyme resulting in autolysis of the gland.
It is important to investigate for the possible causes of Acute pancreatitis before labeling it as 'idiopathic'.
Possible aetiology of Acute pancreatitis :
Gall stones
Alcoholism
Post ERCP
Abdominal trauma
Complication of cardiothoracic, biliary and abdominal surgery
Hypercalcemia
Hyperparathyroidism
Pancreatic Divisum
Autoimmune pancreatitis
Scorpion bite
Drugs : Corticosteroids, Azathioprine, Thiazide diuretics
Mumps, Cocksakie viral infection
Idiopathic
History
Both males and females are equally affected.
Age of onset is around 4th - 5th decade of life.
History of any gall stone diseases, or alcoholism is important (2 most important cause)
Though rare, but ask for recent contact with children with mumps or cocksakie infection.
Symptoms are usually triggered after consumption of large meal or alcohol.
Patient usually complains of sudden onset of severe, continuous epigastric pain, which typically radiates to the back, relieved by bending forwards.
It's accompanied by excessive vomiting and retching, with persistent nausea in between.
Breathing and movements exacerbates the pain.
General examination
Patient appears ill, with shallow breathing.
If the patient looks pale, diaphoretic, it is likely that it has complicated as a hypovolemic shock.
There might be mildly tinged jaundice if the pancreatitis is caused by gall stones.
Even 2-3 days after the illness, the mild tinged jaundice can be caused by compression of biliary duct by edematous head of pancreas.
Shock features of tachycardia, hypotension.
Low grade fever may or may not present.
Abdominal examination
In acute pancreatitis, the complains of the patient may indicate severe pain, but there is usually minimal findings
during abdominal examination.
On inspection, if there's haemorrhagic pancreatits, there might be bruising (bluish purplish) discolouration over around the umbilicus (Cullen's sign) or left flank (Grey Turner's sign).
However, these signs are rarely seen nowadays.
The abdomen may not rise and fall with respiration, since the musculature is tightly contracted, and during onset of paralytic ileus.
Often there is accumulation of inflammatory exudates within the lesser sac, which eventually forms pseudocyst, suggested by epigastric fullness (distension), dullness during percussion over it.
Shifting dullness may be present, bowel sound may be reduced if there is pancreatic ascites.
Invesitgations
Acute pancreatitis is usually diagnosed by typical clinical presentation and laboratory investigation that reveals elevated serum amylase level. Serum amylase of 3-4 times greater than the normal level is suggestive of pancreatitis.
However, if serum lipase assay is available, it is more sensitive and specific.
Note that normal serum amylase level doesn't rule out Acute pancreatitis, and the level poorly correlates with the severity.
Both Ranson's and Glasgow's criteria is used to grade the severity of Acute pancreatitis.
If 3 or more factors are present in the patient, it indicates severe pancreatitis.

Chest X ray, and plain abdominal X ray is not very helpful in the diagnosis of Acute pancreatitis
During early stages, if abdominal X ray is taken, non-specific signs such as Sentinel loop, Renal Halo sign or Colon cut off sign may be present.

Chest X ray may reveal pleural effusion, or if there is diffuse alveolar infiltrates, indicates ARDS.
Though Abdominal USG is non-diagnostic for Acute pancreatitis, but it must be done within 24 hours of presentation.
This is to rule out Acute cholecystitis as a differential diagnosis, to check whether the bile duct is dilated and to reveal any stones within the CBD (gall stone as a cause of Pancreatitis)
CT abdomen is not indicated in every patient.
Only when :
1) Diagnostic uncertainty
2) Severe pancreatitis
3) Clinical deterioration, with multi-organ failure, sepsis
4) Local complications occurs
Complications
Management
a) Conservative
1) Gain IV access and rapid fluid resuscitation.
2) Give analgesics (usually IM pethidine is given)
3) Nil by mouth
4) Insertion of NG tube to relieve vomiting
5) Enteral feeding - nasojejunal tube (to maintain adequate nutrition)
6) Urinary catheterization is done
7) Monitor pulse, BP, urine output and CVP
8) Give antibiotics to prevent secondary infection
b) Endoscopic
If gall stone is strongly suspected as the cause of pancreatitis, the stones should be removed by basket (dormia) through endoscopic sphincterotomy.
If there is severe pancreatitis, or cholangitis occurs, both sphinterotomy and ERCP is done.
c) Surgery
Only indicated if : clinical deterioration during conservative management, unsure diagnosis, local complication occurs.
Adenocarcinoma of Pancreas
More common in males.
Age of presentation - 55-75 years old
85% of CA pancreas involves the head of pancreas, where the prognosis is usually poor.
Patients usually dies within 1 year of diagnosis (5 year survival is exceptional)
Upon presentation, most have progressed to a surgically incurable stage.
Though uncommon, but tumour arising from the distal CBD, duodenum and ampulla has a better outlook.
Currently, the risk factor of developing CA pancreas is thought to be :
Cigarette smoking
High fat and protein diet
Clinical features
Any elderly patient presents with painless jaundice, always suspect the possibility of Pancreatic cancer.
Typical symptoms are usually : Abdominal pain, jaundice and weight loss.
Jaundice is usually obstructive in nature, suggested by the classical triad of pruritus, clay-coloured stool and tea-coloured urine.
There might be steatorrhoea.
Abdominal pain - constant, dull aching, discomfort, over the epigastric region
Sought for symptoms of metastases
On examination, the gall bladder may be palpable, as accordance to the Curviosier's law, which states that,
"For patients presenting with clinically evident jaundice, and on examination the gall bladder is palpable, the cause is more likely to be due to Carcinoma of the Head of Pancreas".
Look for scleral icterus, hepatomegaly, etc.
Investigations
If stool occult blood test is positive, suggestive of a ampullary tumour.
Abdominal USG - usually done to look for liver metastases, or any mass lesion over the pancreas, and dilated bile ducts
CT abdomen - extent of metastases
To confirm the nature of obstruction, MRCP is preferred over ERCP since the former is less invasive.
Surgery of choice : Whipple's procedure
Thursday, May 6, 2010
Peptic ulcer disease and Gastric Carcinoma
Both duodenal ulcers and benign gastric ulcers are believed to be related to mucosal infection by H.pylori.
Peptic ulcer disease are mainly classified as complicated and uncomplicated.

Benign gastric ulcer/duodenal ulcer
Age of presentation ranges from 20-60 years old, which is of course, more common among young adults.
Incidence is higher in males.
Most patients during acute presentation will present with epigastric discomfort or pain.
The intensity ranges from mild dyspepsia (related to food intake, sensation of indigestion), to severe epigastric pain, which often forces the patient to lie down still.
However, as the course of illness goes chronic, pain is rarely severe.
A characteristic feature is night pain, which is a dull, boring ache often wakes patients from sleep.
This is due to the increased gastric acidity at night, and there is lack of food to buffer against it.
The pain either radiates to the back, or towards the RHC (depends on the position of the ulcer : posterior part of stomach, duodenum)
Patient may complain of heart burn, excessive salivation (water/acid brash) related to food intake.
In duodenal ulcer, food intake relieves the symptoms. Hence, patient rarely losses appetite.
In gastric ulcer, food intake aggravates the pain and often patient is apprehensive towards food.
Hence, history of appetite and weight loss is more common in them.
Vomiting relieves the pain in gastric ulcer.
The symptoms exhibit another characteristic, which is periodicity.
As the symptoms persisted for a few weeks, then it may be followed by a period of remission for weeks to months, only to recur after that.
Hemetemesis and malena must be asked in the history as well.
History of drug intake is important, eg : NSAIDs, steroids, salicylates
Other risk factors : Period of stress, cigarette smoking
Often, in examination, apart from abdominal tenderness (guarding if severe), and pallor if there's chronic silent bleeding, there is usually no other significant findings in examination.
Investigation
Full blood count and iron studies may reveals iron deficiency anemia.
Other blood investigations - hypokalemia, increased hematocrit as a result of vomiting.

The choice of imaging in peptic ulcer disease is oesophago-gastroduodenoscopy (OGDS).
Not only it allows visualization of the lesion, it allows mucosal specimens to be biopsied.
Usually biopsy is taken from the gastric antrum, and the specimen is subjected to CLO test.

CLO test consists of inoculating the specimen into a medium containing urea.
Hence, if the specimen contains H.pylori, which produces urease.
The enzyme reacts with urea, and produces ammonia, which changes the medium from yellow to pink/red colour.
That confirms the positive status of H.pylori in the patient.
Management
Due to the finding of Peptic ulcer disease is related to H.pylori infection, the management of uncomplicated peptic ulcer disease is mainly medical.
First of all, avoid smoking, alcohol, and NSAIDs.
However, if the patient requires long courses of NSAIDs, and his/her H.pylori status is -ve, a least damaging agent should be used, such as ibuprofen.
Anti-secretory agents such as proton pump inhibitors, H2 blockers are used.
To supplement these agents, drugs like sucralfate, bismuth compounds, prostaglandin analogues are used.
Eradication of H.pylori
Regardless whether it's a duodenal ulcer/gastric ulcer, once the patient is H.pylori positive, eradication regime of H.pylori is employed.
Usually consist of 1 proton pump inhibitor and 1 or more antibiotics.
In case of duodenal ulcer, if the patient is compliant to the medication, the success rate of remission is about 90%.
Without the eradication regime, the chances of relapse within 1 year is about 80%.
Any persistence of symptoms, a urea breath test (non-invasive) should be done to reassess the H.pylori status in the patient.
However, it must be done 4 weeks after completion of the eradication regime.
Or else, the therapy merely suppresses the bacteria, and may lead to a false negative test result.
However, in gastric ulcer, biopsy need to be taken before making a diagnosis of benign gastric ulcer.
Then if found benign, eradication therapy is given to all patients with +ve status of H.pylori.
Surveillance of the lesion need to be done until the ulcer heals.
Any persistence of symptoms, further biopsy must be taken.
Perforated peptic ulcer
Occasionally, the gastric juices erodes through the gastric/duodenal wall to the extent that only covering left is the visceral peritoneum. The gastric juices collects within the peritoneal cavity, leading to chemical peritonitis.
Eventually, there'll be secondary bacterial infection, leading to spontaneous bacterial peritonitis.
History
Age of presentation : Usually 40-60 years old
History of drug intake : NSAIDs, Steroids, Salicylates
Symptoms :
Sudden onset of severe, continuous abdominal pain which initially confines to the epigastrium.
It rapidly increases in it's intensity, and eventually the pain becomes generalized.
Breathing, movements aggravates the abdominal pain.
Also ask for previous peptic ulcer disease, or history of dyspepsia.
General Examination :
Patient usually lies still on bed, breaths shallowly, and is in a state of distress.
Temperature is usually normal, there might be tachycardia.
On abdominal examination :
On inspection, the abdomen doesn't rise and fall with respiration.
This is due to the tight contraction of the abdominal musculature.
On palpation, abdominal tenderness and guarding initially confines towards the epigastrium.
Later, if the peritonitis becomes generalized, the entire abdomen is tender, and there is intense guarding.
This results in the abdomen being described of having board-like rigidity.
It is impossible to palpate for the abdominal viscus since the muscles are tightly contracted.
On percussion, there may be obliteration/diminished liver dullness (due to the air escaped from the perforated viscus into the peritoneal cavity.
Shifting dullness may be +ve.
On auscultation, bowel sound may be reduced, which indicates generalised peritonitis.
Note : 4-6 hours later, due to the dilution of the accumulated gastric juices within the peritoneal cavity, the patient's symptoms and signs subsides, and the patient actually thought that his/her condition is improving. This is mainly due to the onset of hypovolemic shock, which may be indicated by the presence of increasing abdominal distension, tachycardia, signs of dehydration and etc.
Investigation

In 60% of the patients, the CXR reveals air-filled under the diagphram.
However, absent of this finding does not exclude perforation.
Lateral Chest X-ray may be useful in case an erect CXR is not feasible (patient may be in the state of shock, disability)
In laboratory investigation, there is usually some degree of elevated serum amylase level.
However, 3-4 folds elevated serum amylase level is more suggestive of pancreatitis.
Management
1) Give fluid resuscitation
2) Analgesic for relief of pain
3) IV unasyn and flagyl
4) Anti-emetics are given
5) Insertion of NG tube, and catheterize the patient (monitoring of urine output)
Only after the patient is stable, surgical intervention is done.
In case of a perforated duodenal ulcer, usually simple closure is performed by using an omental patch.
However, if it's a perforated gastric ulcer, a biopsy need to be taken first (to rule out malignancy)
Then, close the perforation by either simple closure or local excision.
During post-op period, IV gastric anti-secretory agent is given.
Pyloric stenosis
First of all, lets take a look at some causes of gastric outlet obstruction :
Peptic ulcer disease
Malignancy (Stomach, pancreas and lymphoma)
Crohn's disease of duodenum
Inflammation of surrounding structures
Gastroparesis (autonomic neuropathy)
Adult hypertrophic pyloric stenosis
 Patients with long standing peptic ulcer disease may develop pyloric stenosis due to healing of the ulcer via fibrosis at the level of the antrum.
Patients with long standing peptic ulcer disease may develop pyloric stenosis due to healing of the ulcer via fibrosis at the level of the antrum.
Usually, the complaints are :
Early satiety
Sensation of fullness, constant epigastric discomfort/pain
History of weight loss
Projectile vomiting is classical, which consists of non-bilious, undigested food particles.
It usually occurs when the patient is lying down, and following the vomiting, it relieves the sensation of fullness.
On examination, the usual findings includes :
On inspection - epigastric distension, visible peristalsis
On palpation - succussion splash ('splashing' sound heard while the abdomen is shaked right-left-right)
Investigation of choice is by OGDS, to determine the nature of obstruction (notice that the symptoms mimics malignancy)
Note that not all patients requires surgical intervention.
A course of PPI can be given first, in hope that when the ulcer heals, the stenosis is resolved.
However, if not reponsive, surgical options includes :

Pyloroplasty or Gastrojejunostomy
Gastric carcinoma
One of the most common cause of death in men.
Pernicious anemia, gastric polyps and chronic gastric ulcers are known pre-malignant conditions.
 Risk factors :
Risk factors :
1) Diet
High intake of salt, nitrosamines (usually present in preservatives)
Gastric CA is more prevalent in countries which malnutrition is a problem.
High intake of vitamin C and E seems to be protective.
2) History of surgery : Gastroenterostomy
3) Type A blood group
4) Atrophic gastritis secondary to Pernicious anemia
5) Chronic gastric ulcer
6) Gastric polyps
History
Age of onset : around 50-70 years of age
Male predominance
Any individual above 45 years of age, presenting with symptoms of dyspepsia, no matter how vague is it, should be investigated.
The epigastric discomfort may not be always associated with food intake.
Patient with long standing history of peptic ulcer disease may notice the change in the character of pain.
Usually it's the periodicity of pain becoming more constant.
There's usually complains of early satiety as well.
Another prominent symptom of Gastric CA is significant loss in appetite, which results in loss of weight.
Patient can lose around 10-20 kg of weight within 1-2 months.
If the tumour is present at the region of gastric cardia, patient may report of progressively worsening dysphagia, and eventually it may be worse enough to cause regurgitation of food contents.
If the tumour is present over the gastric outlet, there may be symptoms of gastric outlet obstruction.
Next is to sought the history of the risk factors mentioned above.
And please elicit history suggestive of metastases to the lung, liver, bones, and brain.
Examination
On general examination, the significant findings includes pallor, cachexia and probably jaundice.
Severe wasting is most noticeable over the hands and face.
Presence of jaundice (usually scleral icterus) indicates liver metastases.
Please look for evidence of an enlarged Virchow's node (left supraclavicular node)
On abdominal examination :
Inspection : abdomen is usually scaphoid, due to the severe wasting. Paradoxically, the abdomen may be distended due to malignant ascites.
Palpation : usually reveals deep tenderness over the epigastric region. In thin patients, deep palpation on full inspiration sometimes reveals a hard, irregular mass. Liver may be palpable, which is hard in consistency, knobbly in surface, non-tender.
Percussion : shifting dullness is +ve if there is malignant ascites
On systemic examination : evidence of metastases (pleural effusion, bony tenderness)
Peptic ulcer disease are mainly classified as complicated and uncomplicated.
Benign gastric ulcer/duodenal ulcer
Age of presentation ranges from 20-60 years old, which is of course, more common among young adults.
Incidence is higher in males.
Most patients during acute presentation will present with epigastric discomfort or pain.
The intensity ranges from mild dyspepsia (related to food intake, sensation of indigestion), to severe epigastric pain, which often forces the patient to lie down still.
However, as the course of illness goes chronic, pain is rarely severe.
A characteristic feature is night pain, which is a dull, boring ache often wakes patients from sleep.
This is due to the increased gastric acidity at night, and there is lack of food to buffer against it.
The pain either radiates to the back, or towards the RHC (depends on the position of the ulcer : posterior part of stomach, duodenum)
Patient may complain of heart burn, excessive salivation (water/acid brash) related to food intake.
In duodenal ulcer, food intake relieves the symptoms. Hence, patient rarely losses appetite.
In gastric ulcer, food intake aggravates the pain and often patient is apprehensive towards food.
Hence, history of appetite and weight loss is more common in them.
Vomiting relieves the pain in gastric ulcer.
The symptoms exhibit another characteristic, which is periodicity.
As the symptoms persisted for a few weeks, then it may be followed by a period of remission for weeks to months, only to recur after that.
Hemetemesis and malena must be asked in the history as well.
History of drug intake is important, eg : NSAIDs, steroids, salicylates
Other risk factors : Period of stress, cigarette smoking
Often, in examination, apart from abdominal tenderness (guarding if severe), and pallor if there's chronic silent bleeding, there is usually no other significant findings in examination.
Investigation
Full blood count and iron studies may reveals iron deficiency anemia.
Other blood investigations - hypokalemia, increased hematocrit as a result of vomiting.

The choice of imaging in peptic ulcer disease is oesophago-gastroduodenoscopy (OGDS).
Not only it allows visualization of the lesion, it allows mucosal specimens to be biopsied.
Usually biopsy is taken from the gastric antrum, and the specimen is subjected to CLO test.
CLO test consists of inoculating the specimen into a medium containing urea.
Hence, if the specimen contains H.pylori, which produces urease.
The enzyme reacts with urea, and produces ammonia, which changes the medium from yellow to pink/red colour.
That confirms the positive status of H.pylori in the patient.
Management
Due to the finding of Peptic ulcer disease is related to H.pylori infection, the management of uncomplicated peptic ulcer disease is mainly medical.
First of all, avoid smoking, alcohol, and NSAIDs.
However, if the patient requires long courses of NSAIDs, and his/her H.pylori status is -ve, a least damaging agent should be used, such as ibuprofen.
Anti-secretory agents such as proton pump inhibitors, H2 blockers are used.
To supplement these agents, drugs like sucralfate, bismuth compounds, prostaglandin analogues are used.
Eradication of H.pylori
Regardless whether it's a duodenal ulcer/gastric ulcer, once the patient is H.pylori positive, eradication regime of H.pylori is employed.
Usually consist of 1 proton pump inhibitor and 1 or more antibiotics.
In case of duodenal ulcer, if the patient is compliant to the medication, the success rate of remission is about 90%.
Without the eradication regime, the chances of relapse within 1 year is about 80%.
Any persistence of symptoms, a urea breath test (non-invasive) should be done to reassess the H.pylori status in the patient.
However, it must be done 4 weeks after completion of the eradication regime.
Or else, the therapy merely suppresses the bacteria, and may lead to a false negative test result.
However, in gastric ulcer, biopsy need to be taken before making a diagnosis of benign gastric ulcer.
Then if found benign, eradication therapy is given to all patients with +ve status of H.pylori.
Surveillance of the lesion need to be done until the ulcer heals.
Any persistence of symptoms, further biopsy must be taken.
Perforated peptic ulcer
Occasionally, the gastric juices erodes through the gastric/duodenal wall to the extent that only covering left is the visceral peritoneum. The gastric juices collects within the peritoneal cavity, leading to chemical peritonitis.
Eventually, there'll be secondary bacterial infection, leading to spontaneous bacterial peritonitis.
History
Age of presentation : Usually 40-60 years old
History of drug intake : NSAIDs, Steroids, Salicylates
Symptoms :
Sudden onset of severe, continuous abdominal pain which initially confines to the epigastrium.
It rapidly increases in it's intensity, and eventually the pain becomes generalized.
Breathing, movements aggravates the abdominal pain.
Also ask for previous peptic ulcer disease, or history of dyspepsia.
General Examination :
Patient usually lies still on bed, breaths shallowly, and is in a state of distress.
Temperature is usually normal, there might be tachycardia.
On abdominal examination :
On inspection, the abdomen doesn't rise and fall with respiration.
This is due to the tight contraction of the abdominal musculature.
On palpation, abdominal tenderness and guarding initially confines towards the epigastrium.
Later, if the peritonitis becomes generalized, the entire abdomen is tender, and there is intense guarding.
This results in the abdomen being described of having board-like rigidity.
It is impossible to palpate for the abdominal viscus since the muscles are tightly contracted.
On percussion, there may be obliteration/diminished liver dullness (due to the air escaped from the perforated viscus into the peritoneal cavity.
Shifting dullness may be +ve.
On auscultation, bowel sound may be reduced, which indicates generalised peritonitis.
Note : 4-6 hours later, due to the dilution of the accumulated gastric juices within the peritoneal cavity, the patient's symptoms and signs subsides, and the patient actually thought that his/her condition is improving. This is mainly due to the onset of hypovolemic shock, which may be indicated by the presence of increasing abdominal distension, tachycardia, signs of dehydration and etc.
Investigation
In 60% of the patients, the CXR reveals air-filled under the diagphram.
However, absent of this finding does not exclude perforation.
Lateral Chest X-ray may be useful in case an erect CXR is not feasible (patient may be in the state of shock, disability)
In laboratory investigation, there is usually some degree of elevated serum amylase level.
However, 3-4 folds elevated serum amylase level is more suggestive of pancreatitis.
Management
1) Give fluid resuscitation
2) Analgesic for relief of pain
3) IV unasyn and flagyl
4) Anti-emetics are given
5) Insertion of NG tube, and catheterize the patient (monitoring of urine output)
Only after the patient is stable, surgical intervention is done.
In case of a perforated duodenal ulcer, usually simple closure is performed by using an omental patch.
However, if it's a perforated gastric ulcer, a biopsy need to be taken first (to rule out malignancy)
Then, close the perforation by either simple closure or local excision.
During post-op period, IV gastric anti-secretory agent is given.
Pyloric stenosis
First of all, lets take a look at some causes of gastric outlet obstruction :
Peptic ulcer disease
Malignancy (Stomach, pancreas and lymphoma)
Crohn's disease of duodenum
Inflammation of surrounding structures
Gastroparesis (autonomic neuropathy)
Adult hypertrophic pyloric stenosis

Usually, the complaints are :
Early satiety
Sensation of fullness, constant epigastric discomfort/pain
History of weight loss
Projectile vomiting is classical, which consists of non-bilious, undigested food particles.
It usually occurs when the patient is lying down, and following the vomiting, it relieves the sensation of fullness.
On examination, the usual findings includes :
On inspection - epigastric distension, visible peristalsis
On palpation - succussion splash ('splashing' sound heard while the abdomen is shaked right-left-right)
Investigation of choice is by OGDS, to determine the nature of obstruction (notice that the symptoms mimics malignancy)
Note that not all patients requires surgical intervention.
A course of PPI can be given first, in hope that when the ulcer heals, the stenosis is resolved.
However, if not reponsive, surgical options includes :
Pyloroplasty or Gastrojejunostomy
Gastric carcinoma
One of the most common cause of death in men.
Pernicious anemia, gastric polyps and chronic gastric ulcers are known pre-malignant conditions.
1) Diet
High intake of salt, nitrosamines (usually present in preservatives)
Gastric CA is more prevalent in countries which malnutrition is a problem.
High intake of vitamin C and E seems to be protective.
2) History of surgery : Gastroenterostomy
3) Type A blood group
4) Atrophic gastritis secondary to Pernicious anemia
5) Chronic gastric ulcer
6) Gastric polyps
History
Age of onset : around 50-70 years of age
Male predominance
Any individual above 45 years of age, presenting with symptoms of dyspepsia, no matter how vague is it, should be investigated.
The epigastric discomfort may not be always associated with food intake.
Patient with long standing history of peptic ulcer disease may notice the change in the character of pain.
Usually it's the periodicity of pain becoming more constant.
There's usually complains of early satiety as well.
Another prominent symptom of Gastric CA is significant loss in appetite, which results in loss of weight.
Patient can lose around 10-20 kg of weight within 1-2 months.
If the tumour is present at the region of gastric cardia, patient may report of progressively worsening dysphagia, and eventually it may be worse enough to cause regurgitation of food contents.
If the tumour is present over the gastric outlet, there may be symptoms of gastric outlet obstruction.
Next is to sought the history of the risk factors mentioned above.
And please elicit history suggestive of metastases to the lung, liver, bones, and brain.
Examination
On general examination, the significant findings includes pallor, cachexia and probably jaundice.
Severe wasting is most noticeable over the hands and face.
Presence of jaundice (usually scleral icterus) indicates liver metastases.
Please look for evidence of an enlarged Virchow's node (left supraclavicular node)
On abdominal examination :
Inspection : abdomen is usually scaphoid, due to the severe wasting. Paradoxically, the abdomen may be distended due to malignant ascites.
Palpation : usually reveals deep tenderness over the epigastric region. In thin patients, deep palpation on full inspiration sometimes reveals a hard, irregular mass. Liver may be palpable, which is hard in consistency, knobbly in surface, non-tender.
Percussion : shifting dullness is +ve if there is malignant ascites
On systemic examination : evidence of metastases (pleural effusion, bony tenderness)
Wednesday, May 5, 2010
Gall Stones
Pathophysiology
Mostly cholesterol stones (80%), pigment stones or mixed stones.
Whether cholesterol remains as solution within bile depends on it's concentration, and the levels of phospholipids and bile acids within.
If the bile is supersaturated by cholesterol, and/or levels of phospholipids and bile acids is low, this promotes formation of cholesterol crystals.
These cholesterol crystals are toxic towards the gall bladder musculature, and hence damages it.
This results in gall bladder hypomotility, and enhances the nucleation of theses gall bladder crystals.
Eventually, gall stones are formed.
As for pigment stones, there are 2 types, namely black and brown stones.
Black stones are sterile stones, usually caused by extensive hemolysis leading to unconjugated hyperbilirubinemia. Eg, seen in Hereditary Spherocytosis, Sickle-cell disease.
Whilst brown stones are non-sterile stones, mainly caused by infection.
Eg, certain bacteria (E.coli) produces B-glucoronidase, which converts conjugated bilirubin back to unconjugated bilirubin.
Also associated with parasitic worm infestation, eg : Ascariasis, Clonorchis sinensis
Complications
1) Gall bladder
Biliary colic
Acute cholecystitis
Chronic cholecystitis
Empyema
Mucocele
Perforation
2) Biliary tract
Biliary tract obstruction
Acute pancreatitis
Ascending cholangitis
3) Intestine
Gall stone ileus
Acute cholecystitis
Usually caused by obstruction of cystic duct by gall stones, leading to gall bladder distension, chemical inflammation, and eventual bacterial infection.
History
Age : Typically 30-60 years old. Presentation in younger patients, may be due to Congenital hemolytic anemia
Gender : Females are more commonly affected
Symptoms :
Fever
Sudden onset of severe, continuous RHC pain
Radiates to the back (close to the inferior angle of right scapula)
Associated with nausea and vomiting
Duration of pain usually exceeds 3-6 hours
Pain aggravated by movements and breathing
May have previous h/o of flatulent dyspepsia or biliary colic
On general examination :
Patient appears ill
Lying still on bed, breathing shallowly
Tachycardia +ve, Pyrexia +ve
During initial stages of inflammation - RHC fullness (known as Zackary-cope's sign)
RHC tenderness, guarding/rigidity, +ve Murphy's sign
Before the onset of guarding, during the early stages the gall bladder may be palpable
If the inflammation persisted for a few days, with subsequent subside of symptoms, an inflammatory mass may be palpable (empyema)
Boas Sign +ve
Biliary colic
Before proceeding to investigations of Acute cholecystitis, briefly about biliary colic.
It's actually a misnomer, caused by spasm of gall bladder musculature, trying to force the stone down the cystic duct.
Since it's a visceral pain, pain is usually felt over the epigastrium (foregut)
The pain is typically aggravated by intake of oily food.
Since after ingesting oily food, as it passes through the 2nd part of duodenum, it stimulates the production of cholecystikinin from the duodenal mucosa.
It causes contraction of the gall bladder musculature over the stones, hence causing pain.
Duration of pain typically lasted < 3 hours.
However, in practice, patient usually localizes their pain poorly (c/c usually diffuse upper abdominal pain)
It's a pseudocolic, since there's no complete relief of pain in between periods of excruciating exacerbations.
There might be nausea and vomiting.
On examination, there may be tachycardia, but fever is absent.
On abdominal examination, other than tenderness, guarding, usually there's no other signs.
Hence, there's a frequent overlap in between the clinical features of biliary colic and acute cholecystitis.
Here the table showing their difference :
 Investigations
Investigations
Full blood count - reveals leucocytosis
Abdominal X ray - not useful, only 10-15% of the calculus is visible through plain abdominal X ray
USG abdomen - visualisation of gall bladder wall, contents, biliary tree
Management
As for asymptommatic gall stones, which is usually detected incidentally, the best option is to observe (no further intervention)
However, prophylactic cholecystectomy will be indicated in :
a) Non-functioning gall bladder
b) Gall bladder with calcified/thickened wall
c) Diabetic patients (prevent Emphysematous Cholecystitis)
d) Multiple small stones (risk of stones rolling into CBD)
e) Congenital hemolytic anemia
During acute presentation, > 90% of the cases, symptoms subsides with conservative management :
1) Nil by mouth
2) Administration of analgesics
3) Administration of antibiotics (Unasyn + Flagyl)
4) Gain IV access, give IV fluids
5) Monitoring of vital signs
6) If symptoms subsided, initially oral fluid intake is allowed, then followed by fat-free diet, and lastly regular diet
7) USG - to evaluate whether there's any local complications
8) Plan for cholecystectomy
Pre-operative investigations
1) Informed consent
2) Full blood count
3) BUSE/Creatinine
4) Liver function test
5) ECG, Chest X ray (if medically indicated)
6) Antibiotic prophylaxis
7) DVT prophylaxis
Cholecystectomy can be done via laproscopic approach or laparotomy.
Gall stone ileus
Small bowel obstruction caused by gall stone impaction at the distal ileum
Usually seen in females, age > 60 years old, with h/o of recurrent cholecystitis
Erosion of the stones through the duodenum, eventually forming a fistula with the distal ileum
Presentation is similar to any other small bowel obstruction
Plain abdominal X ray reveals multiple air-fluid levels, and there might be aerobilia (gas within biliary tree)
 Soft stones can be crushed
Soft stones can be crushed
Hard stones requires enterotomy
Mirizzi's syndrome
 A complication of cholecystitis
A complication of cholecystitis
Gall stone impaction occurs at cystic duct.
There's impingement of the gall stone over the common hepatic duct, which eventually results in formation of a fistula in between the gall bladder and the bile duct.
An exception towards the Curvoisier's law.
Complications : Post-cholecystectomy
1) Haemorrhage
Usually the source is from cystic artery.
One should suspect possibility of haemorrhage if the patient complains of persistent abdominal pain, or features of hypovolemic shock during post-operative period
2) Infection
Drastically reduced after administration of prophylactic antibiotics before cholecystectomy.
3) Leakage of bile
Usually due to disrupted ligature, or accidental removal of any accessory ducts.
Patient usually complains of persistent abdominal pain.
If there's no biliary ascites -> ERCP
If there's biliary ascites -> Laparotomy
4) Post-cholecystectomy syndrome
5) Biliary stricture
6) Retained stone
Usually found during T-tube cholangiogram
Any procedure done to explore the common bile duct requires insertion of T-tube.
This is to prevent biliary stasis due to formation of stricture.
The opening of bile duct is sutured to the T-tube, which the long limb is brought out through an abdominal stab incision.
Any bile is collected through a bag.
7-10 days later, T-tube cholangiogram is done (iodine as contrast material)
If there's free flow of contrast material into the duodenum, and there's no residual stone -> remove the T-tube
If there's residual stone :
Stone is small - try using normal saline to irrigate the duct via the T tube (stone eventually migrates to the duodenum)
Stone is large - delayed removal after 4-6 weeks, via radiographically guided removal using dormia basket
Mostly cholesterol stones (80%), pigment stones or mixed stones.
Whether cholesterol remains as solution within bile depends on it's concentration, and the levels of phospholipids and bile acids within.
If the bile is supersaturated by cholesterol, and/or levels of phospholipids and bile acids is low, this promotes formation of cholesterol crystals.
These cholesterol crystals are toxic towards the gall bladder musculature, and hence damages it.
This results in gall bladder hypomotility, and enhances the nucleation of theses gall bladder crystals.
Eventually, gall stones are formed.
As for pigment stones, there are 2 types, namely black and brown stones.
Black stones are sterile stones, usually caused by extensive hemolysis leading to unconjugated hyperbilirubinemia. Eg, seen in Hereditary Spherocytosis, Sickle-cell disease.
Whilst brown stones are non-sterile stones, mainly caused by infection.
Eg, certain bacteria (E.coli) produces B-glucoronidase, which converts conjugated bilirubin back to unconjugated bilirubin.
Also associated with parasitic worm infestation, eg : Ascariasis, Clonorchis sinensis
Complications
1) Gall bladder
Biliary colic
Acute cholecystitis
Chronic cholecystitis
Empyema
Mucocele
Perforation
2) Biliary tract
Biliary tract obstruction
Acute pancreatitis
Ascending cholangitis
3) Intestine
Gall stone ileus
Acute cholecystitis
Usually caused by obstruction of cystic duct by gall stones, leading to gall bladder distension, chemical inflammation, and eventual bacterial infection.
History
Age : Typically 30-60 years old. Presentation in younger patients, may be due to Congenital hemolytic anemia
Gender : Females are more commonly affected
Symptoms :
Fever
Sudden onset of severe, continuous RHC pain
Radiates to the back (close to the inferior angle of right scapula)
Associated with nausea and vomiting
Duration of pain usually exceeds 3-6 hours
Pain aggravated by movements and breathing
May have previous h/o of flatulent dyspepsia or biliary colic
On general examination :
Patient appears ill
Lying still on bed, breathing shallowly
Tachycardia +ve, Pyrexia +ve
During initial stages of inflammation - RHC fullness (known as Zackary-cope's sign)
RHC tenderness, guarding/rigidity, +ve Murphy's sign
Before the onset of guarding, during the early stages the gall bladder may be palpable
If the inflammation persisted for a few days, with subsequent subside of symptoms, an inflammatory mass may be palpable (empyema)
Boas Sign +ve
Biliary colic
Before proceeding to investigations of Acute cholecystitis, briefly about biliary colic.
It's actually a misnomer, caused by spasm of gall bladder musculature, trying to force the stone down the cystic duct.
Since it's a visceral pain, pain is usually felt over the epigastrium (foregut)
The pain is typically aggravated by intake of oily food.
Since after ingesting oily food, as it passes through the 2nd part of duodenum, it stimulates the production of cholecystikinin from the duodenal mucosa.
It causes contraction of the gall bladder musculature over the stones, hence causing pain.
Duration of pain typically lasted < 3 hours.
However, in practice, patient usually localizes their pain poorly (c/c usually diffuse upper abdominal pain)
It's a pseudocolic, since there's no complete relief of pain in between periods of excruciating exacerbations.
There might be nausea and vomiting.
On examination, there may be tachycardia, but fever is absent.
On abdominal examination, other than tenderness, guarding, usually there's no other signs.
Hence, there's a frequent overlap in between the clinical features of biliary colic and acute cholecystitis.
Here the table showing their difference :

Full blood count - reveals leucocytosis
Abdominal X ray - not useful, only 10-15% of the calculus is visible through plain abdominal X ray
USG abdomen - visualisation of gall bladder wall, contents, biliary tree
Management
As for asymptommatic gall stones, which is usually detected incidentally, the best option is to observe (no further intervention)
However, prophylactic cholecystectomy will be indicated in :
a) Non-functioning gall bladder
b) Gall bladder with calcified/thickened wall
c) Diabetic patients (prevent Emphysematous Cholecystitis)
d) Multiple small stones (risk of stones rolling into CBD)
e) Congenital hemolytic anemia
During acute presentation, > 90% of the cases, symptoms subsides with conservative management :
1) Nil by mouth
2) Administration of analgesics
3) Administration of antibiotics (Unasyn + Flagyl)
4) Gain IV access, give IV fluids
5) Monitoring of vital signs
6) If symptoms subsided, initially oral fluid intake is allowed, then followed by fat-free diet, and lastly regular diet
7) USG - to evaluate whether there's any local complications
8) Plan for cholecystectomy
Pre-operative investigations
1) Informed consent
2) Full blood count
3) BUSE/Creatinine
4) Liver function test
5) ECG, Chest X ray (if medically indicated)
6) Antibiotic prophylaxis
7) DVT prophylaxis
Cholecystectomy can be done via laproscopic approach or laparotomy.
Gall stone ileus
Small bowel obstruction caused by gall stone impaction at the distal ileum
Usually seen in females, age > 60 years old, with h/o of recurrent cholecystitis
Erosion of the stones through the duodenum, eventually forming a fistula with the distal ileum
Presentation is similar to any other small bowel obstruction
Plain abdominal X ray reveals multiple air-fluid levels, and there might be aerobilia (gas within biliary tree)
Hard stones requires enterotomy
Mirizzi's syndrome
Gall stone impaction occurs at cystic duct.
There's impingement of the gall stone over the common hepatic duct, which eventually results in formation of a fistula in between the gall bladder and the bile duct.
An exception towards the Curvoisier's law.
Complications : Post-cholecystectomy
1) Haemorrhage
Usually the source is from cystic artery.
One should suspect possibility of haemorrhage if the patient complains of persistent abdominal pain, or features of hypovolemic shock during post-operative period
2) Infection
Drastically reduced after administration of prophylactic antibiotics before cholecystectomy.
3) Leakage of bile
Usually due to disrupted ligature, or accidental removal of any accessory ducts.
Patient usually complains of persistent abdominal pain.
If there's no biliary ascites -> ERCP
If there's biliary ascites -> Laparotomy
4) Post-cholecystectomy syndrome
5) Biliary stricture
6) Retained stone
Usually found during T-tube cholangiogram
Any procedure done to explore the common bile duct requires insertion of T-tube.
This is to prevent biliary stasis due to formation of stricture.
The opening of bile duct is sutured to the T-tube, which the long limb is brought out through an abdominal stab incision.
Any bile is collected through a bag.
7-10 days later, T-tube cholangiogram is done (iodine as contrast material)
If there's free flow of contrast material into the duodenum, and there's no residual stone -> remove the T-tube
If there's residual stone :
Stone is small - try using normal saline to irrigate the duct via the T tube (stone eventually migrates to the duodenum)
Stone is large - delayed removal after 4-6 weeks, via radiographically guided removal using dormia basket
Tuesday, January 5, 2010
Intercostal drainage
Indications for intercostal drain :
a) Pneumothorax
b) Traumatic haemopneumothorax
c) Malignant pleural effusion
d) Empyema thoracis / Complicated parapneumonic effusion
e) Post-operative drainage : esophagectomy, cardiac surgery, thoracotomy
Equipments :
Intercostal tube or Chest tube (Size for pneumothorax : 36-40 Fr, hemothorax : 22-24 Fr)

Connecting tubes and compatible connectors
Underwater seal drainage bottle containing water upto mark

Line clamp
11 blade scalpel
Instruments for blunt dissection
Blue and Green needle
2 or 3/0 silk in a large hand-held needle
10ml syringe
20ml of 1% lidocaine
Normal saline
Sterile gloves
Sterile drapes
Sterile gauze
Skin prep. solution

Procedures :
1) Explain procedure to the patient if appropriate.
2) Connect the patient to a pulse oxymeter.
3) Prop up the patient to a semi-recumbent position, with the ipsilateral limb abducted.
4) Prepare the skin at the site of tube insertion (antiseptics)
5) Make proper drapping over field of interest.
6) Infiltrate the local anesthetic sufficiently, including the parietal pleura and the periosteum of the rib posterior to the line of incision.
7) Make a transverse, 2cm incison over the 5th intercostal space, over the mid-axillary line (may extend upto the anterior axillary line)
8) Proceed with blunt dissection until the pleura is visible.
9) Now, gently and firmly, by using a blunt-ended clamp, puncture the pleura, and widened the hole created.
10) Place one of your finger into the hole to ensure there's no adhesions.
11) Insert the chest tube without trochar into the puncture hole created after clamping it. Guide the tube superiorly if it's a pneumothorax, and towards the base if it's a hemothorax.
12) Fix the chest tube using the silk sutures.
13) Connect the distal end of the tube to the underwater seal drainage bottle, and remove the clamp.
Potential complications :
1) Misplacement (intra-parenchymal or subcutaneous)
2) Damaging the surrounding structures : liver, spleen, lungs, heart, aorta, diagphram, etc
3) Surgical emphysema
4) Wound infection, empyema
5) Pain
a) Pneumothorax
b) Traumatic haemopneumothorax
c) Malignant pleural effusion
d) Empyema thoracis / Complicated parapneumonic effusion
e) Post-operative drainage : esophagectomy, cardiac surgery, thoracotomy
Equipments :
Intercostal tube or Chest tube (Size for pneumothorax : 36-40 Fr, hemothorax : 22-24 Fr)
Connecting tubes and compatible connectors
Underwater seal drainage bottle containing water upto mark
11 blade scalpel
Instruments for blunt dissection
Blue and Green needle
2 or 3/0 silk in a large hand-held needle
10ml syringe
20ml of 1% lidocaine
Normal saline
Sterile gloves
Sterile drapes
Sterile gauze
Skin prep. solution
1) Explain procedure to the patient if appropriate.
2) Connect the patient to a pulse oxymeter.
3) Prop up the patient to a semi-recumbent position, with the ipsilateral limb abducted.
4) Prepare the skin at the site of tube insertion (antiseptics)
5) Make proper drapping over field of interest.
6) Infiltrate the local anesthetic sufficiently, including the parietal pleura and the periosteum of the rib posterior to the line of incision.
7) Make a transverse, 2cm incison over the 5th intercostal space, over the mid-axillary line (may extend upto the anterior axillary line)
8) Proceed with blunt dissection until the pleura is visible.
9) Now, gently and firmly, by using a blunt-ended clamp, puncture the pleura, and widened the hole created.
10) Place one of your finger into the hole to ensure there's no adhesions.
11) Insert the chest tube without trochar into the puncture hole created after clamping it. Guide the tube superiorly if it's a pneumothorax, and towards the base if it's a hemothorax.
12) Fix the chest tube using the silk sutures.
13) Connect the distal end of the tube to the underwater seal drainage bottle, and remove the clamp.
Potential complications :
1) Misplacement (intra-parenchymal or subcutaneous)
2) Damaging the surrounding structures : liver, spleen, lungs, heart, aorta, diagphram, etc
3) Surgical emphysema
4) Wound infection, empyema
5) Pain
Subscribe to:
Posts (Atom)